Uterine cancer
Sophie Matzik is a freelance writer for the medical team.
More about the experts All content is checked by medical journalists.Uterine cancer (uterine carcinoma, corpus carcinoma) is a malignant tumor of the uterine body. It almost always develops from the mucous membrane (endometrium) that lines the inside of the uterus. Experts then speak of endometrial cancer. Uterine cancer is the fourth most common cancer in women. Regular check-ups are important in order to discover and treat the tumor in good time. Here you can read everything you need to know about the causes, treatment and prognosis of uterine cancer.
ICD codes for this disease: ICD codes are internationally recognized codes for medical diagnoses. They can be found, for example, in doctor's letters or on certificates of incapacity for work. C55C57C54
Uterine cancer: description
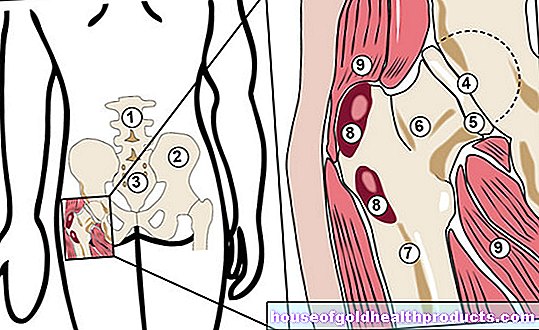
The uterus (uterus) is a muscular hollow organ. The upper part is called the body of the uterus (corpus); the two fallopian tubes flow into it. The lower short and tubular section is called the cervix. It connects the body with the scabbard.
Uterine cancer develops from the upper part of the uterus, the body of the uterus (corpus). This is where the name corpus carcinoma comes from. In contrast to many other types of cancer, uterine cancer usually does not develop from the muscle layer, but from the mucous membrane that lines the inside of the uterus (endometrium). Experts then speak of endometrial cancer.
The lining of the uterus renews itself regularly up to the menopause. Each month the upper layers are shed and expelled with the menstrual period. Changes in the mucous membrane occur during menopause. Individual cells can transform themselves into cancer cells through genetic change (mutation) - an endometrial cancer develops.
Cancer of the uterus should not be confused with cancer of the cervix (cervical cancer). This develops from the lower part of the uterus. Both types of cancer differ in terms of early detection, diagnosis and treatment. Another difference to uterine cancer: Vaccination against HP viruses (human papillopmavirus) is only used to prevent cervical cancer. It does not protect against uterine cancer.
Uterine Cancer: Facts and Figures
Uterine cancer is one of the most common cancers in women. Every year around 12,000 women develop uterine cancer. The mean age of onset is around 68 years; Endometrial cancer rarely occurs before the age of 40. Well over half of those affected develop uterine cancer after the menopause. The chances of a cure and the prognosis are good if the body carcinoma is discovered at an early stage. The majority of the sick can be cured.
Uterine cancer: symptoms
You can read everything you need to know about the typical signs of uterine cancer in the article Uterine cancer - symptoms.
Uterine cancer: causes and risk factors
The exact cause of uterine cancer (endometrial cancer) is still unknown. Scientists suspect that various risk factors interact in its development.
The development of uterine cancer probably depends largely on the female sex hormones, especially estrogen - almost every endometrial cancer is estrogen-dependent in its growth. Before menopause, the hormone ensures that the mucous membrane is regularly renewed. It is produced in the ovaries and adipose tissue. The luteal hormone progesterone (a progestogen) is also produced in the ovaries. It counteracts the regenerative effects of estrogen and also ensures that the mucous membrane is shed with the menstrual period. So if the effects of estrogen outweigh the overgrowth of the endometrium and result in endometrial cancer.
This is why overweight women in particular have an increased risk of developing uterine cancer after the menopause: their ovaries no longer produce a “protective” progesterone, which a lot of adipose tissue still produces estrogen.
Women who had their first menstrual period early or who went through the menopause are also at a slightly higher risk of endometrial cancer. The same applies to women who have never given birth or who have never breastfed.
Treatment with female sex hormones (hormone replacement therapy, HRT) is often used during menopause. These may only be given in combination with progestins in women who still have a uterus.
Age is also a risk factor for uterine cancer.
Genetic factors can also play a role in the development of uterine cancer. A single gene is responsible, and there is a 50 percent chance that it will be passed on to the next generation. In affected families, the risk of uterine cancer is increased as well as that of ovarian and colon cancer.
Certain hormonal imbalances are additional risk factors for uterine cancer. In some women, the lining of the uterus builds up, but there is no ovulation and thus no subsequent progestin formation. Or, for other reasons, the influence of the progestin is too weak to expel the thickened mucous membrane. Such an unusual thickening of the endometrium, unrelated to the normal cycle, is called endometrial hyperplasia. It can occur before and after menopause and lead to endometrial cancer.
Also, uterine cancer can develop after giving an anti-estrogen called tamoxifen. Tamoxifen is widely used in the treatment of breast cancer. Even after radiation treatment, the risk of developing uterine cancer is increased. With these therapies, however, the benefits of treatment with regard to the other cancers are greater than the risk of uterine cancer.
Uterine cancer: examinations and diagnosis
Endometrial cancer can be diagnosed in a number of ways.
The first method of choice is an ultrasound examination of the vagina (vaginal ultrasound). The gynecologist can also feel changes in the mucous membrane by palpation. It is often necessary to take a tissue sample (biopsy). This is examined in the laboratory. In this way it can be determined whether there is a benign or malignant change and what stage the uterine cancer is.
A hysteroscopy can confirm the suspicion of uterine cancer. This procedure is carried out on an outpatient basis. A small rod (hysteroscope) is inserted into the uterus through the vagina. A sample of the mucous membrane can also be taken without any problems.
Imaging can be used to assess the spread of uterine cancer. Magnetic resonance imaging (MRT) and computed tomography (CT) are available for this purpose. These examinations are carried out in the hospital.
If it is suspected that the uterine cancer is no longer confined to the uterus, further examinations will be carried out. For example, a cystoscopy and a rectoscopy are used to check whether the tumor has spread to the bladder or the intestine.
Uterine cancer: treatment
The most important therapeutic measure for uterine cancer is surgery. Depending on the aggressiveness and stage of the cancer, other treatments can be added, such as chemotherapy. Another option for treating uterine cancer is hormone therapy in certain cases.
Uterine cancer: surgery
In most cases of endometrial cancer, surgery is the best treatment option. How much tissue is removed depends on the stage of the cancer. If the uterine cancer has not spread too much, the uterus, fallopian tubes and ovaries are removed.
In more advanced stages, it may also be necessary to cut out the lymph nodes in the pelvic area and along the abdominal artery, the tissue around the uterus and part of the vaginal vault. If the tumor has already spread to the bladder or intestine, more tissue must be removed.
Only in exceptional situations is an operation for uterine cancer avoided in favor of other treatment methods. This is the case, for example, if the operation would be too risky - for example because the woman's general condition is very poor or if she has previous illnesses such as severe cardiovascular disease. Hormone therapy may also be attempted first in pre-menopausal women who are still determined to have children.
Uterine cancer: radiation therapy
Radiation therapy after the uterine cancer operation is indicated if the vaginal vault has also been affected by the cancer. This is to prevent the tumor from recurring. Radiation is also given if the uterine cancer is too advanced for surgery or has not been completely removed.
Uterine cancer: chemotherapy
If the uterine cancer cannot be operated on, if there is a high risk of relapse after the operation, or if a new tumor has already developed, chemotherapy is given. The appropriate medication is administered to the patient by infusion. In some cases, a combination of chemotherapy and radiation therapy can be useful.
Uterine cancer: hormone therapy
As part of hormone therapy for uterine cancer, patients receive artificial luteal hormones (progestins), mostly in tablet form. They should counteract the effects of estrogen to such an extent that the growth of the estrogen-dependent tumor is inhibited - but the disease often progresses anyway. A cure cannot be achieved with hormone therapy.
Hormone treatment is therefore usually only used for uterine cancer when neither surgery nor radiation therapy is possible. Even in women who would like to have a child, tumor growth can be slowed down with the help of the hormones at least until pregnancy becomes possible. After the delivery, doctors usually recommend removing the uterus because of the high risk of relapse.
Uterine cancer: disease course and prognosis
Five years after being diagnosed with uterine cancer, around 80 percent of patients are still alive (five-year survival rate). In individual cases, the prognosis depends on various factors. In addition to the general state of health, the stage in which the body carcinoma is at the time of diagnosis has an influence on the chances of recovery:
If the uterine cancer is detected early and therapy is started immediately, the prognosis is good. It becomes more difficult, however, if the uterine tumor has already formed daughter tumors (metastases). These tend to settle in the lungs or bones and are more difficult to treat. It is therefore important that every woman see a doctor immediately and have the cause clarified if she has any symptoms of uterine cancer (bleeding outside of the menstrual period or after the menopause).
Fear of relapse
After surviving uterine cancer, some women are very worried that the tumor could recur. This psychological stress can significantly impair the performance and quality of life of those affected. Regular check-ups, psychological support and discussions in a self-help group for women with uterine cancer can help!
Tags: toadstool poison plants parasites laboratory values