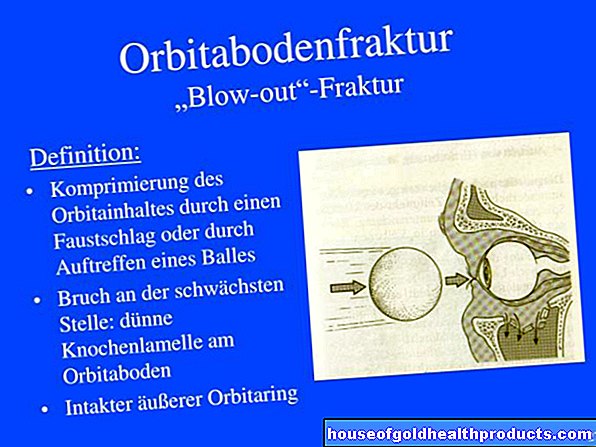
Plantar fasciitis
Dr. med. Mira Seidel is a freelance writer for the medical team.
More about the experts All content is checked by medical journalists.Plantar fasciitis (also: plantar fasciitis) is an inflammation of the tendon plate of the sole of the foot and is typically triggered by overuse. The tendon plate attachment to the calcaneus is usually affected. Plantar fasciitis manifests itself as pain in the heel, which occurs mainly when there is pressure and strain. Read everything you need to know about the causes and treatments for plantar fasciitis.
ICD codes for this disease: ICD codes are internationally recognized codes for medical diagnoses. They can be found, for example, in doctor's letters or on certificates of incapacity for work. M72
Plantar fasciitis: description
Plantar fasciitis is the most common cause of chronic heel pain (calcaneodynia). It can put a considerable strain on the patient.The plantar fascia, the tendon plate under the foot that is inflamed in plantar fasciitis, arises from the lower and front edge of the calcaneus, the so-called calcaneal tuberosity. It connects the tarsal, metatarsal and metatarsal joints. Everything together forms the longitudinal arch of the foot ..
When the foot rolls, the plantar fascia is put under tension by the so-called windlass effect, which ensures the transmission of force from the forefoot to the rear foot. The fascia has the task of tensioning the longitudinal arch, aligning the rear and forefoot, absorbing shocks and passively lifting the arch of the foot.
The term plantar fasciitis is based on the Anglo-American term "plantar fasciitis". Pathologically and anatomically, however, the symptoms correspond to the "heel pain syndrome", while "plantar fasciitis" means a clinical picture that takes place over the second sphenoid and metatarsal bones.
The term “heel spur” is usually used incorrectly. A heel spur is a bony spur on the heel bone (calcaneus) in the attachment area of the tendon plate of the sole of the foot (plantar fascia). It is often an incidental finding on a lateral x-ray of the foot. It is associated with plantar fasciitis, but not its cause and is usually symptom-free. So the heel spur does not trigger the heel pain, but the plantar fasciitis.
Plantar fasciitis: symptoms
The onset of plantar fasciitis is insidious. Over time, symptoms gradually worsen, usually over weeks or months. Initially, the symptoms only occur during exercise, later also in the morning when you get up and at rest. They can lead to the inability to walk. A sign of plantar fasciitis is pain in the heel immediately after getting up, but it disappears after a short walk. When exercising, those affected initially feel painful episodes at the beginning of the exertion, which decrease as they warm up. Symptoms return towards the end of the workout. Sprinting and jumping in particular increase the pain.
Plantar fasciitis: causes and risk factors
Plantar fasciitis is mainly caused by overloading the plantar fascia. This can occur during sport, especially when running or jumping. Plantar fasciitis is particularly common in the fourth and fifth decades of life, which is probably related to age-related wear and tear. About ten percent of all athletes in the running disciplines are affected by plantar fasciitis. Other high-risk sports include basketball, tennis, soccer and dancing. However, there is no connection between the duration of the training and the frequency of the complaints.
If the fascia at the base (insertion tendinopathy) becomes inflamed as a result of excessive stress, discomfort can occur. Excessive stress can be caused, for example, by a shortened Achilles tendon. Bursitis (bursitis) in the area of the plantar fascia attachment can also cause pain in this area.
Furthermore, injuries can be the cause of plantar fasciitis. Even the smallest changes can damage the collagen fibers and lead to chronic inflammation. For example, patients report having their heel caught on the curb when crossing the street.
Plantar fasciitis: examinations and diagnosis
If you suspect plantar fasciitis, you can see a general practitioner or an orthopedic specialist. Plantar fasciitis has a characteristic medical history (anamnesis), which means that the diagnosis can be made quickly. Typical questions the doctor may ask during the anamnesis interview could be:
- Did you have an acute foot injury?
- Does it hurt under the heel when put under pressure?
- When does the pain occur? In which movements?
- When is the pain most severe? When do they subside?
- Where is the pain radiating to?
During the examination, the patient usually reports localized tenderness under the heel at the attachment point of the fascia. A rupture would show a bruise on the sole of the foot with tenderness to pressure.
If the symptoms are acute, it is likely a strain or - rarely - a tear of the plantar tendon. The person concerned stated that he had to stop exercising immediately and that walking was no longer possible due to the pain, or that the symptoms worsened. Sometimes a swelling or bruise can also indicate other injuries such as fractures, muscle injuries, or a tear.
Plantar fasciitis: imaging diagnostics
In addition to X-rays, ultrasound and magnetic resonance tomography are used for the imaging diagnosis of plantar fasciitis.
Plantar fasciitis diagnosis: X-ray
Side x-rays show about 50 percent of patients with plantar fasciitis to have heel spurs. However, this is not a diagnostic criterion and is seen in about 25 percent of the population on x-rays. In order to rule out a malalignment of the rear foot, X-rays of the foot are made in three planes.
Plantar Fasciitis Diagnosis: Ultrasound
In the case of plantar fasciitis, a thickened plantar fascia can be seen in the longitudinal section on ultrasound. The plantar fascia is three to four millimeters thick in a healthy person, while in plantar fasciitis the fascia layers are often thickened to seven to ten millimeters.
Plantar fasciitis diagnosis: magnetic resonance imaging
With the help of magnetic resonance imaging (MRT), precise cross-sectional images of the foot can be made. A contrast agent that is injected into the vein is usually used so that the doctor can make a better judgment. The exact localization and extent of the inflammation can be determined with the MRI. The use of MRI is particularly useful before an operation, so as not to overlook possible fractures, partial fractures, tendon abnormalities and bone contusions.
Plantar fasciitis: treatment
Plantar fasciitis is one of the most persistent and frustrating sports injuries. Although there are many conservative and surgical treatment options, plantar fasciitis can easily become chronic.
Plantar Fasciitis Treatment - Conservative
In order to reduce the inflammation and the pain of plantar fasciitis, the treatment initially consists of relieving the strain or adjusting the physical activity. The training methods and circumstances, such as mountain runs, running surfaces made of sand or rubble, sudden training increases, must be analyzed and changed if necessary.
Stretching exercises: For the calf and sole muscles, stretching exercises are an essential part of the conservative treatment of plantar fasciitis. In one study, 72 percent of patients improved symptoms with stretching alone. For example, a stretching exercise consists of rolling your foot over a bottle filled with ice. Passively flexing the foot with a towel, which is wrapped around the forefoot and pulled towards the head, is also a good stretching exercise. It is best to repeat the stretches about three times a day for at least ten minutes.
Shoe insoles: Shoe insoles that support and straighten the longitudinal arch directed towards the middle of the body and relieve the fasciae have a positive effect. Night positioning splints with the ankle in the extended position help especially with severe pain in the morning.
Physiotherapy: Special massages such as transverse friction massages at the tendon insertion are initially uncomfortable, but help relieve pain.
Medication: Non-steroidal anti-inflammatory drugs can be used as medication. Injection therapy with cortisone is another option; up to 70 percent of the pain should disappear. However, repeated injections can reduce the metabolism of the tendon tissue so much that the risk of rupture increases significantly.
Extracorporeal shock wave therapy (ESWT): In extracorporeal shock wave therapy, ultrasonic shock waves are brought into the injured region via the skin. The method has become increasingly important because of its success in physical therapy for improving movement and reducing pain. However, since the treatment costs are very high, only chronic cases and cases that do not respond to other conservative measures are initially treated.
X-ray inflammation radiation: The so-called X-ray inflammation radiation is also used for plantar fasciitis that has been unsuccessfully treated conservatively and causes freedom from pain in around two thirds of the patients treated with it. The disadvantage, however, is the radiation exposure.
Surgical plantar fasciitis treatment
If, in rare cases, none of the conservative measures help after six months and the symptoms remain unchanged, an operation can be considered. However, this should be reserved for cases that do not respond to conservative treatment attempts - around five percent of all patients with plantar fasciitis have to undergo surgery.
Open notch
The open notch is the standard surgical treatment for plantar fasciitis. The plantar fascia is notched at the origin using a short, inclined skin incision above the point on the sole of the foot that is painful to pressure. In this way, painful scarring can be avoided. If there is a heel spur, it can be removed at its base. Endoscopic treatment is also possible. The healing time is therefore usually shorter.
A lower leg splint should be worn for about two days after the operation. After that, it is important to use a careful partial load in the first few days, whereby special insoles should be used. Physiotherapy with a specific foot muscle strengthening and stretching program is also required.
After the sixth postoperative week, the running load can be increased slowly, although initially only light endurance training is recommended. Jump loads should be strictly avoided before the tenth to twelfth postoperative week. The entire healing process takes at least twelve weeks after an operation, in individual cases even up to a year.
Surgery complications
As a complication, the pain can persist after an operation or move to the metatarsus. This happens when the entire plantar fascia has been severed because the tension in the longitudinal arch has changed. As with any operation, general operational risks such as superficial or deep infections, painful scars or deep vein thrombosis cannot be ruled out.
Plantar fasciitis: disease course and prognosis
The majority of patients with plantar fasciitis are successfully cured with conservative treatment methods. However, the course of plantar fasciitis can be lengthy and last one to two years. During this time, an athlete must severely limit his or her workload. After surgical treatment, around nine out of ten patients, including athletes, report an improvement in their symptoms of 80 percent.
Tags: menshealth nourishment home remedies