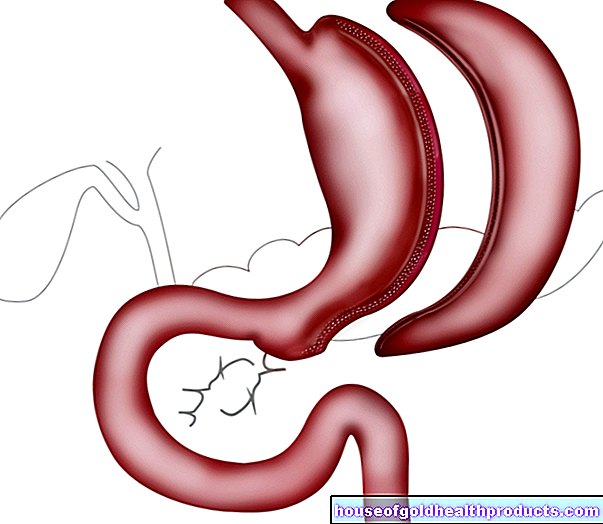
Living with diabetes
and Martina Feichter, medical editor and biologist Updated onMartina Feichter studied biology with an elective subject pharmacy in Innsbruck and also immersed herself in the world of medicinal plants. From there it was not far to other medical topics that still captivate her to this day. She trained as a journalist at the Axel Springer Academy in Hamburg and has been working for since 2007 - first as an editor and since 2012 as a freelance writer.
More about the experts All content is checked by medical journalists.
Living with diabetes requires some adjustments from the patient. Going on vacation spontaneously or drinking a glass of wine unplanned is often not possible without further ado. But if diabetics take some advice to heart and make certain preparations, they too can enjoy everyday life with almost no restrictions. Here you can find out everything you need to know about living with diabetes and what you need to consider.
ICD codes for this disease: ICD codes are internationally recognized codes for medical diagnoses. They can be found, for example, in doctor's letters or on certificates of incapacity for work. E11E10E13O24H36E12E14
Traveling with diabetes
Discuss your travel destination with your doctor, especially if you are planning a long-haul trip. It is also advisable to have addresses of German-speaking doctors in the country of travel to hand. For diabetics who want continuous medical care even while on vacation, many tour operators now have appropriate offers.
Find out about the climate and current temperatures in your holiday destination before you start your journey. Pack appropriate clothing: it should be loose, comfortable and made of natural fibers.
Make sure you choose your shoes and stockings carefully to avoid chafing and blisters. Prefer comfortable shoes without seams. Choose cotton material for your stockings that absorbs sweat better. Inspect your feet every night for injuries and bruises.
Important documents and records
Get the "Diabetes Health Passport" (issued by the German Diabetes Society, DDG), if you don't already have it, and take it with you on your trip. When traveling to a foreign-language country, we recommend an international diabetic pass in several languages or one in the national language of the travel destination. An international diabetic emergency ID card is also very useful. It is available, for example, as a download on the homepage of the Diabetes Information Service in Munich (www.diabetesinformationsdienst-muenchen.de).
Diabetics also need a medical certificate stating that they medically justify carrying medication, insulin syringes, pens, lancets, glucagon sets, etc. The attending physician should fill out this certificate - preferably in other languages (such as English) depending on the travel destination.
Don't forget your vaccination card either!
Medicines and accessories for diabetes therapy
Before you start your journey, work out the amount of diabetes medication (blood sugar-lowering tablets, insulin) you will need for the entire holiday (or ask your doctor about this). In this case, it is best to take twice as much with you - in case you lose something or your stay is unexpectedly extended.
Also take into account that you may need to adjust the dose of diabetes medication to suit your vacation activities. Perhaps you are more active and exercise more than at home (muscle work reduces the need for insulin). Or you just relax on the beach most of the time (less muscle work - the need for insulin increases). Therefore, test your blood sugar more often while traveling. Before you start your journey, discuss any dose adjustments that may be necessary with your doctor, for example in the context of larger time differences (see below: Air travel).
Put your diabetic medication together in a medication plan, on which the names of the active substances and the dosage are noted (or ask your doctor to do so). With the help of the active ingredient names, you can also obtain the right medication in an emergency abroad. It is better, however, to take sufficient medication with you from home (see below).
When packing, think about important accessories for diabetes therapy such as:
- Blood sugar measuring device (including spare batteries), possibly reserve device
- Blood sugar test strips
- Blood sugar diary
- Acetone test strips
- Lancing device and lancets
- Insulin syringes, insulin pump with cannulas or pump accessories (plus spare batteries)
- Glucagon emergency kit (if you have a tendency to severe hypoglycaemia)
- Blood pressure monitor (for diabetics with high blood pressure)
In addition, you should always have glucose with you (even when you are not traveling). It is a quick help with hypoglycaemia. Glucose juices within easy reach are also handy.
Make sure you store your medication properly throughout the trip. This is especially true for insulin. It should be stored between +2 and +8 degrees Celsius (vegetable compartment in the refrigerator) whenever possible. To protect against excessive heat, you can store the insulin in, for example, styrofoam, in a cooler bag or in a thermos that you have rinsed out beforehand with cold water.
Insulin vials / cartridges that are currently in use can be safely stored at room temperature for up to four weeks. However, do not expose them to extreme heat or direct sunlight. To protect against the cold (e.g. during winter sports), you should carry the insulin close to your body, e.g. in a belt pocket under your sweater.
If insulin gets too hot it will get flaky, cloudy, and grainy and may stick to the edge of the vial. It can also turn yellowish-brownish in color (e.g. from exposure to sunlight). Do not use this insulin anymore! Ask your doctor or pharmacist for advice if you are unsure.
Some of the other contents of the first-aid kit are also temperature-sensitive. Protect your blood glucose meter and the test strips from large temperature fluctuations and also from high humidity. The reaction of the test strips is linked to a certain temperature.
By the way: Your first-aid kit naturally also includes the usual preparations and utensils recommended for travel. These include, for example, preparations for gastrointestinal problems (such as motion sickness, diarrhea, constipation), plasters and compresses, disinfectants, etc. Your doctor can advise you on putting together your first-aid kit.
Air travel
The diabetes medication belongs in hand luggage: on the one hand you need them during the trip, on the other hand the checked baggage could get lost. In addition, the temperature in the aircraft's hold can drop so much that, for example, the insulin freezes - then it can no longer be used! Accessories that you need every day, such as blood glucose meters, insulin pumps, lancets, etc. belong in hand luggage. You can take this and the medication with you on board with a medical certificate.
Inquire with your airline in advance about any requirements and restrictions. Often the insulin pen has to be given to the flight attendants for safekeeping on board. As soon as you need it, however, you will of course be given it.
Bring enough of your own food and drinks (especially carbohydrates) with you on the plane. Then you avoid hypoglycaemia if, for example, no food can be served due to turbulence or the flight takes longer than planned and nothing is served.
If you are flying over several time zones, you should discuss with your doctor in advance how much you need to adjust your medication. This is especially true for insulin therapy. Here are some general recommendations:
- During the flight and afterwards, blood sugar should be measured every two to three hours.
- Sometimes it can be safer to set your blood sugar level a little higher than usual to avoid hypoglycemia.
- Time differences of up to four hours (in both directions) usually do not require any significant adjustments to the insulin therapy.
- Flights to the west (day longer and therefore need higher): a normal dose of insulin before the flight. During the flight, possibly fast-acting insulin (for example with high blood sugar, increased carbohydrate intake, etc.). After arrival, insulin injections at the usual time (new time zone!).
- Flights to the east (day shorter and therefore less need): a reduced insulin dose before the flight. During the flight, insulin dosage depending on the measured blood sugar value. Upon arrival, insulin injections at the usual time (new time zone!).
These recommendations are only of a general nature. Your doctor can give you different tips, tailored to your personal state of health.
nourishment
Fortunately, many diabetics nowadays no longer have to orientate themselves towards the food on offer when choosing a holiday destination - intensified insulin therapy (ICT) is now widespread. Type 2 diabetics on pills have also gained more leeway - with drugs that work quickly with meals.
Rigid eating rules on vacation only exist for diabetics who are still using conventional insulin therapy with clearly defined insulin doses.
Diabetics should find out about the typical foods and their carbohydrate content before starting their journey - if possible. To be on the safe side, take a BE table with you and measure your blood sugar more often, especially with unclear foods.
Drink enough! In general, about 1.5 to two liters of non-alcoholic fluids per day is recommended. In warmer countries you should even drink three to four liters of non-alcoholic liquid (exception: diabetics with heart and kidney disease!).
The same applies to alcohol when traveling as at home (see below): Always consume it in moderation and, preferably, never on an empty stomach, but together with a carbohydrate-rich food. This is how you avoid hypoglycaemia.
Vaccination protection and malaria prophylaxis
Check your vaccination protection, especially against tetanus, diphtheria and polio. Depending on the travel destination, further vaccinations may be useful or even mandatory (such as yellow fever vaccination, typhoid vaccination, etc.). Get advice from your doctor or a tropical medicine specialist. Take care of this in good time before you start your journey, because some vaccinations require a certain amount of time in advance.
The doctor or tropical medicine specialist can also inform you about any malaria prophylaxis that may be necessary.
Diabetes and alcohol
Alcohol is a cell poison that attacks various organs in the body that may have already been damaged by diabetes mellitus. In addition, diabetics, whose liver is busy with alcohol detoxification, are acutely exposed to the risk of hypoglycaemia. It is therefore particularly important for people with diabetes to know the effects of alcohol on the body.
Hypoglycaemia
Normally, the liver is constantly releasing small amounts of sugar into the blood to keep the brain and muscles energized. Alcohol inhibits this release of sugar. This lowers the blood sugar level. In combination with diabetes medication, it can easily lead to low blood sugar (hypoglycaemia). As a countermeasure, the body would actually release the hormone glucagon. It releases the sugar stored in the liver. But that too is prevented by alcohol.
Alcohol consumption can therefore trigger significant hypoglycaemia in diabetics - even for several hours afterwards, because the effect of alcohol lasts for a long time. If a sharp drop in blood sugar occurs during sleep, it can even be life-threatening for the diabetic.
Obesity
One gram of alcohol has almost as many calories as one gram of fat. Diabetics in particular should therefore only consume the “calorie bomb” alcohol with caution. Because being overweight lowers the cells' sensitivity to insulin and increases the body's need for insulin. Especially diabetics who are already overweight should best avoid alcohol altogether.
Nervous system
Alcohol and diabetes are the two main causes of damage to the nerve tract (peripheral polyneuropathy). When both factors come together, the nerves are damaged twice. The damage mostly affects the nerve tracts of the feet and often causes diabetic foot syndrome.
impotence
Alcohol affects potency. Diabetes mellitus can also lead to impotence through damage to blood vessels and nerves. Diabetics who suffer from sexual disorders should therefore better avoid alcohol.
heart
Alcohol in excess damages the heart in several ways. For example, regular alcohol consumption can lead to high blood pressure. This damages the blood vessels and increases the risk of cardiovascular diseases (such as heart attacks and strokes). The same applies to disorders of lipid metabolism, which are also favored by alcohol. In addition, alcohol can trigger cardiac arrhythmias and damage the heart muscle cells, so that a heart muscle disease (cardiomyopathy) develops.
Diabetes mellitus also endangers heart health. Vascular damage caused by excessively high blood sugar can impair the blood flow to the heart muscle. The possible consequences are coronary artery disease (CHD) and heart attack.
The heart is even more at risk when alcohol and diabetes occur in combination.
pancreas
The pancreas is particularly sensitive to alcohol. It is the main cause of inflammation of the organ (pancreatitis). Acute pancreatitis is life-threatening. If it is chronic, it runs in flares of inflammation and can lead to a loss of function of the pancreas. This is fatal because only this organ can produce insulin.
Diabetics with diseases of the pancreas should therefore not consume alcohol. This is even more the case for diabetics who only needed insulin as a result of acute or chronic pancreatitis.
Since the pancreas also produces important digestive juices, damage to the organ leads to serious digestive disorders and vitamin deficiencies.
liver
Alcohol and fatty liver disease, which is very common in overweight diabetics, together lead to scarring and ultimately to a loss of liver function. One speaks here of "fatty liver cirrhosis". Alcohol and diabetes also work together unfavorably here.
Medication
Many drugs are metabolized by the liver. If the liver is not fully functional, some drugs accumulate in the body and cause undesirable side effects. Conversely, some drugs are excreted more quickly due to the breakdown of alcohol and no longer achieve the desired effect. Particular attention should be paid to this in the case of diabetes mellitus requiring medication or insulin.
Use of alcohol in moderation
Diabetics are allowed to drink alcohol, but should follow a few rules. Type 2 diabetics in particular should not drink alcohol regularly.
- Always consume alcohol with foods containing carbohydrates. The blood sugar-lowering effect of alcohol can be balanced or at least mitigated by the carbohydrates. This reduces the risk of hypoglycaemia.
- The risk of hypoglycaemia can be exacerbated if other blood sugar-lowering factors are added to alcohol consumption. These are, for example, sports, dancing or long-term avoidance of food.
- Do not inject any additional insulin for the consumption of "hard" alcoholic beverages (such as schnapps, vodka), wine and possibly also beer. If you want to drink sweet cocktails, mulled wine etc., an extra dose of insulin may be useful. Discuss this with your doctor in advance!
- Do not drink large quantities of non-alcoholic beers. They hardly contain any alcohol (less than 0.5 percent), but they contain a lot of malt sugar and thus unfavorable carbohydrates.
- Check your blood sugar more frequently while you drink alcohol and in the hours after it. Hypoglycaemia can occur ten to 20 hours after drinking alcohol! To be on the safe side, inform family and friends about the potential risk of hypoglycaemia.
- If you sleep soundly, you will not notice a drop in blood sugar caused by alcohol. Therefore, before lying down it may be useful to eat carbohydrates that slowly increase blood sugar (such as whole grain products, potatoes). In any case, you should check your blood sugar before going to bed!
Do not drink alcohol if you are pregnant, have diabetic nerve damage (diabetic nephropathy), or already have liver or pancreas problems. It is also recommended to abstain from alcohol completely in the case of disorders of the lipid metabolism (such as increased cholesterol levels) and a tendency to hypoglycaemia.
Diabetes and pregnancy
A diabetic, like any other woman, can give birth to healthy children - provided she receives medical care before and during pregnancy. If the diabetes is not optimally adjusted during pregnancy, this can be dangerous for the developing child and the mother-to-be.
What can you do yourself?
At least three months before the onset of a (planned) pregnancy, an HbA1c value should be aimed for, which is ideally below 6.5 percent (but at least below 7.0 percent).
Pregnant diabetics should measure their blood sugar before each meal and one to two hours afterwards. These measured values should be within a certain range for the child's healthy development - just like the measurements taken before going to bed and at night. The following target values are recommended:
|
Time of measurement |
Blood sugar in mg / dl |
Blood sugar in mmol / l |
|
sober / before meals |
65 to 95 |
3.6 to 5.3 |
|
1 hour after eating |
< 140 |
< 7,7 |
|
2 hours after eating |
< 120 |
< 6,6 |
|
before bedtime |
90 to 120 |
5.0 to 6.6 |
|
at night (2 a.m. to 4 a.m.) |
> 60 |
> 3,3 |
|
mean blood glucose (MBG) |
85 to 105 |
4.7 to 5.8 |
Frequent blood sugar checks are very important, especially with unstable type 1 diabetes.
All women (including non-diabetics) should ensure that they have an adequate supply of folic acid. This prevents child malformations (such as "open back"). A daily intake of 0.4 to 0.8 milligrams of folate is recommended at least four weeks before the (planned) pregnancy and until the end of the 12th week of pregnancy. In addition, pregnant women should eat a diet rich in folate (with green leafy vegetables, legumes, whole grain products, etc.).
A sufficient supply of iodine is also very important for the health of mother and child. Pregnant diabetics should therefore take a preparation containing at least 200 micrograms of iodide per day as a preventive measure. A diet rich in iodine and the use of iodized table salt are also recommended.
Pregnant diabetics are advised to have additional ultrasound examinations in order to detect possible growth disorders in the child at an early stage.
You should clarify secondary diseases of diabetes before you become pregnant and, if necessary, have them treated by a doctor (e.g. diabetic nephropathy). A very common complication in pregnant diabetics is retinal disease (diabetic retinopathy). If the eyes are still okay, diabetics should see an ophthalmologist before a (planned) pregnancy, immediately after the onset of pregnancy and then every three months until the birth. If there are already changes in the retina, the doctor can arrange more frequent check-ups with the diabetic.
General tips that are recommended for every pregnant woman (including non-diabetic women) are:
- Do not smoke. Also avoid secondhand smoke.
- Refrain from alcohol completely.
- Only take any medication (including herbal supplements) if absolutely necessary and on medical advice. Also discuss the intake of dietary supplements with your doctor in advance.
ICT or insulin pump?
In principle, both therapies are equivalent. Patients under intensive conventional insulin therapy (ICT) can be adjusted just as easily as with insulin pump therapy.
The need for insulin changes during pregnancy. From the second trimester of pregnancy, it increases continuously (by 50 to 100 percent until birth). This is especially true for type 2 diabetics who are very overweight (obese). At the beginning of the birth, however, the need for insulin often drops drastically. This makes it necessary to adjust the insulin therapy again. During pregnancy and after delivery, blood sugar must therefore be measured more frequently than usual. Diabetics can find out from their doctor whether and how they need to adjust their insulin dosages.
What are the risks?
A pregnancy with type 1 and type 2 diabetes is generally considered a risk pregnancy. With careful medical supervision and good metabolic control, the risk of complications can be reduced.
Important complications and risks for mother and child are, for example:
- In the first trimester of pregnancy, diabetics have an increased risk of low blood sugar (hypoglycaemia).
- The risk of early miscarriage (premature abortion) is increased in type 1 and type 2 diabetics. It depends on the metabolic control before conception (higher risk with poorly controlled blood sugar).
- The risk of malformations in children is increased in diabetics, also depending on the metabolic setting before conception. On average, it is around four times as high as in the general population and is therefore just under nine percent. The most common malformations of the heart and vessels close to the heart, neural tube defects (such as "open back") and multiple (multiple) malformations occur.
- The unborn child can grow unusually large (macrosomia), which can cause problems during vaginal delivery. A caesarean section is then often necessary.
- Even if they are unusually large (macrosomia), newborns of diabetics are often "immature" in terms of the development of individual organs. This is especially true of the lungs.
- There is a risk of hypoglycaemia in the child immediately after birth. Regular blood sugar tests in the child within the first few days and any glucose administration, however, usually reduce serious health consequences for the baby.
- Pregnant diabetics are more prone to infections of the genital tract and urinary tract. Such urogenital infections can increase the risk of premature birth.
- Maternal high blood pressure can only develop during pregnancy or exist before it. If the expectant mother also excretes protein in the urine (proteinuria) and has water retention (edema), preeclampsia ("pregnancy poisoning") is present. It can be dangerous for mother and child (possible complications are eclampsia, HELLP syndrome).
- An existing diabetic retinopathy (diabetic retinopathy) can worsen during pregnancy (usually in the 3rd trimester).
- Mild diabetic kidney disease (diabetic nephropathy) can increase the risk of preeclampsia and miscarriage. Advanced nephropathy carries a high risk for the unborn / newborn (premature birth, stillbirth, delayed growth, psychomotor developmental delays in childhood).
For both type 1 and type 2 diabetics, delivery must be planned in a perinatal center with at least level 2. There the maternity ward is directly connected to a newborn intensive care ward (at least four beds). As an expectant mother, you should see the perinatal center by the 36th week of pregnancy at the latest.
Tags: drugs digital health laboratory values