osteoporosis
and Martina Feichter, medical editor and biologistSophie Matzik is a freelance writer for the medical team.
More about the expertsMartina Feichter studied biology with an elective subject pharmacy in Innsbruck and also immersed herself in the world of medicinal plants. From there it was not far to other medical topics that still captivate her to this day. She trained as a journalist at the Axel Springer Academy in Hamburg and has been working for since 2007 - first as an editor and since 2012 as a freelance writer.
More about the experts All content is checked by medical journalists.
Osteoporosis (bone loss) is one of the most important common diseases. Millions of people in Germany suffer from it, especially older women. In those affected, the bone substance is increasingly broken down. This makes the bones more and more unstable and fragile. Read everything you need to know about the causes, symptoms, therapy and prevention of osteoporosis here!
ICD codes for this disease: ICD codes are internationally recognized codes for medical diagnoses. They can be found, for example, in doctor's letters or on certificates of incapacity for work. E24M81M80
Brief overview
- What is osteoporosis? Metabolic disease of the bones in which more and more bone tissue is broken down (bone loss). This makes it easier for the bones to break.
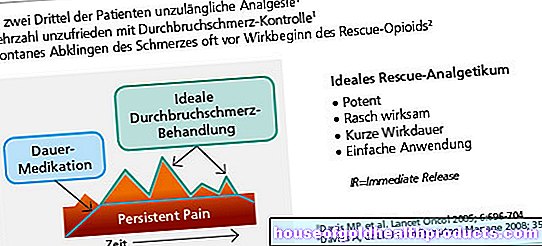
- Symptoms: often no symptoms at first. In the further course persistent pain such as back pain, broken bones in the case of minor injuries or for no apparent reason (spontaneous fractures), increasing hunched back ("widow's hump") and decreasing body size.
- Causes: Primary osteoporosis occurs in old age and after the menopause (lack of estrogen!). Secondary osteoporosis is the result of other diseases or medication (hyperthyroidism, cortisone, etc.).
- Treatment: non-drug measures such as adequate exercise (sport, physiotherapy) and proper nutrition; Calcium and vitamin D supplements; Osteoporosis drugs (bisphosphonates etc.); Treatment of underlying diseases (for secondary osteoporosis); possibly surgery for broken bones
- Prognosis: So far, osteoporosis is not curable. Early diagnosis and treatment is all the more important. Otherwise, the bone loss will continue to progress. This then means increasing pain and increased bone fractures.
What happens with osteoporosis?
Bones consist of two basic building blocks:
- a special fabric that gives them shape and stability (matrix)
- various minerals that are stored in the matrix (mainly calcium and phosphate). They condense and strengthen the structure.
The bones are constantly being remodeled to adapt to changing requirements. Up to around the age of 35, more bone mass is usually built up than broken down. From the age of 35 onwards, bone loss gradually predominates and accelerates with age. Healthy elderly people lose around 0.5 to 1 percent of their bone mass every year.
This normal bone metabolism can be disrupted by a wide variety of influences. For example, a lack of calcium, a lack of exercise and hormone-related diseases can cause bone formation to be inhibited and / or bone loss to be promoted. As a result, the bone mass shrinks - osteoporosis develops. Older people are mainly affected. In extreme cases, patients can lose up to six percent of their bone mass per year!
This is how the bone changes in osteoporosis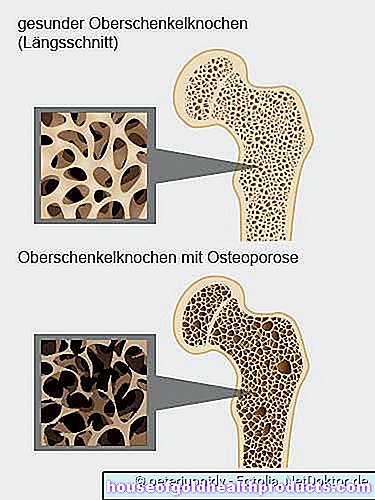
Osteoporosis: Who Does It Affect?
Osteoporosis usually occurs in old age. In Germany, around a quarter of all people over the age of 50 have osteoporosis. That's about 7.8 million people.
-
"Strength training strengthens the bones"
Three questions for
Prof. Dr. med. Dietmar Daichendt,
General practitioner and osteologist -
1
Is osteoporosis a disease at all?
Prof. Dr. med. Dietmar DaichendtYes, bone loss has been declared by the WHO (World Health Organization) to be one of the ten most important widespread diseases in the western world. It affects far more women than men. As a precaution, a bone density determination is recommended for women aged 55 and over and men aged 60 and over in order to be able to take countermeasures in good time. But: not everyone gets osteoporosis. It depends largely on genetic and hormonal factors as well as lifestyle habits.
-
2
Why is exercise so important in osteoporosis?
Prof. Dr. med. Dietmar DaichendtBecause movement, especially physical exertion, transmits the muscle power exerted to the periosteum via the tendons. This in turn transmits the stimulus to the bony cortex and strengthens it. Strength training has a positive effect on the bony cortex, but unfortunately not on the inside of the bone. Its condition is largely dependent on the hormones estrogen (in women) and testosterone (in men). Movement can therefore at least partially help stabilize the bones.
-
3
To what extent do I have to adjust my lifestyle if I have osteoporosis?
Prof. Dr. med. Dietmar Daichendt
As mentioned, do strength training, drink calcium-rich mineral water - this is one of the healthiest sources of calcium - and often in the sun to get vitamin D. Both are important for bone strength. However, there are only a few people who raise their vitamin D levels sufficiently with sunlight alone. That is why vitamin D is also useful as a dietary supplement. A blood test can determine if this is necessary.
-
Prof. Dr. med. Dietmar Daichendt,
General practitioner and osteologistProf. Daichendt runs the "Osteoporosis Center" in Munich, the first exclusively osteoporosis focus center founded in Germany.

There is a difference between the sexes: Around every third woman after the menopause and every fifth older man suffer from bone loss.
Almost all patients (95 percent) have what is known as primary osteoporosis: It is caused either by the lack of estrogen after menopause (in women) or by increased bone loss in old age (both sexes).
Only in a few osteoporosis patients (5 percent) is bone loss the result of other diseases or medication (secondary osteoporosis). More than half of those affected are men.
Special form: transient osteoporosis
A special form of the disease is the so-called transient osteoporosis. Middle-aged men in particular suffer from it. But women in the last trimester of pregnancy are also more often affected.
Transient osteoporosis is a rapidly progressing, painful breakdown of bone near the joints. Usually the hip joint is affected. The patients have severe pain in the joint. This is also restricted in its mobility.
Transient osteoporosis can be clearly diagnosed using magnetic resonance imaging (magnetic resonance imaging, MRI). In the vicinity of the joint, extensive swelling (edema) in the bone marrow can be detected. Transient osteoporosis is viewed as a reaction to this local bone marrow edema. That is why it is also known as bone marrow edema syndrome.
What exactly triggers the development of transient osteoporosis is not known. Circulatory disorders in the bones, overloading of the hip joints and trauma (such as a fall on the hip) are discussed.
The most important therapeutic measure is to completely relieve the affected joint.Then in most cases the disease heals spontaneously within several months (provided there are no complications such as a broken bone). The pain can be relieved with medication (such as ibuprofen).
According to current knowledge, transient osteoporosis does not lead to permanent (chronic) symptoms.
Osteoporosis: symptoms
Osteoporosis usually develops slowly. At the beginning, those affected generally have no complaints. Only in the further course does pain arise, for example back pain and knee pain. They are often not recognized as the first symptom of osteoporosis.
Some patients also have fractures: they are often the result of minor injuries. Even a small, harmless fall can result in a broken forearm. Spontaneous fractures for no apparent reason are also possible first symptoms of osteoporosis.
In the advanced stage of osteoporosis, there is an increased incidence of unreasonable fractures. Typical osteoporosis symptoms often turn out to be broken bones near the hips (such as femoral neck fractures), fractures of the upper and lower arm and the vertebral body (vertebral body fracture).
Vertebral fractures
Sometimes vertebral bodies slowly collapse in osteoporosis. Those affected often do not notice anything. These “creeping breaks” do not cause any pain. As a result, they are often not recognized and left untreated. However, they cause the body to decrease in size. If there are multiple vertebral body fractures, it can even shrink by several centimeters! In addition, a hunched back can develop ("widow's hump").
Acute vertebral fractures are also possible signs of osteoporosis. In contrast to creeping fractures, pain does occur, and clearly. In addition, mobility is significantly restricted in everyday life.
In general, the following symptoms can indicate vertebral body invasions:
- severe, local, stabbing to burning back pain
- persistent back pain
- Decrease in height
- Hunchback
Femoral neck fracture
Femoral neck fractures are among the most serious complications of osteoporosis. Symptoms such as severe pain in the hip joint and a misalignment of the affected leg indicate such a femoral neck fracture. In addition, the affected hip joint can no longer be loaded.
Vicious circle
With every broken bone, the risk of further fractures increases. For fear of renewed fractures, osteoporosis patients often become insecure and anxious when walking and often support themselves. This increases the risk of falling.
In addition, muscle strength dwindles with age. In addition, many older people can hear and see more difficultly. This affects the balance, which increases the risk of falling. This increases the risk of fractures even further. Those affected get into a vicious circle of fear and insecurity, increased risk of falling and new bone fractures, which further ignite the fear.
Osteoporosis: causes and risk factors
There are basically two groups of osteoporosis: primary osteoporosis and the much rarer secondary osteoporosis.
Primary osteoporosis: causes
Primary osteoporosis occurs in women after the menopause and in both sexes at an older age:
Bone loss after menopause (postmenopausal osteoporosis) is hormonal: the female sex hormones (estrogens) regulate the formation and effect of calcitonin and vitamin D. These two hormones are important for building bones. During the menopause, the production of estrogen decreases. This is why many women develop bone loss after their last menstrual period (menopause).
Sex hormones (such as testosterone) are also important for bone metabolism in men. However, they do not stop producing testosterone in middle age. This is why osteoporosis is less common in men than in women.
As we get older, everyone increasingly loses bone mass. This can cause osteoporosis in both men and women. Doctors speak of senile osteoporosis here.
Overall, various risk factors favor the development of osteoporosis. Diet that is not very bone-friendly (e.g. low-calcium diet) and lack of exercise are the first to be mentioned here.
A nutritional deficiency in calcium and vitamin D leads to bone loss, especially from the age of 70. Excessive diets, excessive coffee consumption, the abuse of laxatives and too much phosphate in food mean that the bones do not receive enough calcium and vitamin D. This promotes osteoporosis.
Excessive alcohol and nicotine consumption are also considered risk factors for bone loss.
In addition, osteoporosis occurs more frequently in certain families. Experts therefore suspect that genetic factors also play a role.
Secondary osteoporosis: causes
In contrast to primary osteoporosis, secondary osteoporosis is the result of other diseases or their treatment (medication).
For example, secondary osteoporosis can be caused by too much cortisone in the body. Such an excess of cortisone results either from diseases such as Cushing's syndrome or from long-term therapy with cortisone.
An overactive thyroid (hyperthyroidism) can also trigger osteoporosis: the excess of thyroid hormones accelerates the metabolism and promotes bone breakdown. If the parathyroid is overactive, osteoporosis is also common. This is because too much parathyroid hormone is released. This hormone is an antagonist of calcitonin and vitamin D: It releases calcium from the bones and thus promotes their breakdown.
Other secondary causes of osteoporosis are:
- hormone-related diseases such as underactive sex glands (ovaries, testicles), overactive adrenal cortex, type 1 diabetes
- Stomach and intestinal diseases such as Crohn's disease, ulcerative colitis, lactose intolerance, celiac disease: the utilization of important nutrients such as calcium is impaired.
- malignant tumors (such as bone metastases)
- Severe chronic kidney failure (renal insufficiency): The body excretes a lot of calcium. So that the calcium level in the blood does not drop too much, calcium is released from the bones and absorbed into the blood.
- Inflammatory rheumatic diseases such as rheumatoid arthritis ("rheumatism")
- other diseases such as anorexia or cirrhosis of the liver (malnutrition promotes osteoporosis)
- Medication: In addition to cortisone, other medications can also promote osteoporosis, for example anticonvulsants (anti-epileptic drugs), cyclosporine (after organ transplants, for skin diseases, etc.), heparin (long-term therapy to prevent thrombosis) and certain hormone therapies (e.g. for prostate cancer).
Osteoporosis: examinations and diagnosis
At the slightest suspicion of osteoporosis such as a broken bone for no apparent reason (spontaneous fracture), you should see a doctor. The earlier the bone loss is treated, the sooner the progression of the disease can be stopped. In addition, a basic diagnosis of osteoporosis is recommended for all people with an increased risk of bone fractures. It consists of several parts:
Doctor-patient conversation
First, the doctor will collect the patient's medical history (anamnesis) in conversation with the patient. The doctor asks about the general condition of the patient. He also asks whether there are any complaints or restrictions in everyday life. These include, for example, back pain, difficulty climbing stairs, lifting heavy objects or pain when running for a long time.
Information about any broken bones or falls in the past is also important for the doctor. In addition, the doctor asks whether the patient suffers from an illness or is using medication.
Physical examination
This is followed by a physical exam. The doctor also measures the patient's height and weight.
Tests are used to check physical fitness and mobility. An example is the "timed-up-and-go" procedure:
In doing so, the doctor stops the time it takes the patient to get up from a chair, walk ten feet, turn around, walk back and sit down again. He may also use any walking aids that he otherwise uses in everyday life.
If the patient takes more than 30 seconds to complete the task, his mobility is likely to be impaired. Then there is an increased risk of falling.
Measurement of bone density
Another important component of osteoporosis diagnosis is bone density measurement (osteodensitometry, DXA measurement). With the help of low-dose X-rays, the bone density in the lumbar spine, the entire thigh bone and the femoral neck is determined. The measured values (T values) are compared with the typical mean values in the respective age group. If they are 2.5 units or more below the age-typical mean values, the definition of osteoporosis is fulfilled: The patient has bone loss.
Overall, the World Health Organization (WHO) differentiates between four stages of bone loss, depending on the T value of the bone density measurement:
- Grade 0: osteopenia. In this preliminary stage of osteoporosis, the mineral content of the bones is reduced by a value of 1 to 2.5.
- Grade 1: osteoporosis. The mineral content of the bones is reduced by more than 2.5. Broken bones (fractures) are not yet present.
- Grade 2: Manifest osteoporosis. It occurs when the bone mineral content is reduced by more than 2.5 and the patient has already had one to three vertebral fractures.
- Grade 3: advanced osteoporosis. All patients who have bone mineral content more than 2.5 units below the average and who have multiple (multiple) vertebral body fractures have advanced osteoporosis.
X-ray examination
Any broken bones (fractures) can be seen on an X-ray. Among other things, vertebral body fractures often occur in osteoporosis. They can arise from a one-off event (such as a fall) or be the result of long-lasting, subliminal mechanical influences.
In the second case, there are creeping breaks. They cause the vertebral body in question to deform. Experts refer to this as sintering or creep deformation. The following applies: the stronger the deformation, the more pronounced the osteoporosis. This can be determined by measuring the vertebral body heights between the fourth thoracic vertebra and the fifth lumbar vertebra using X-rays. The measured value obtained (vertebral deformity score) shows how pronounced the osteoporosis is.
Blood tests
As part of the diagnosis of osteoporosis, the patient's blood is also examined. On the one hand, a blood count is taken. Other parameters are also determined, for example liver and kidney values as well as calcium and phosphate levels. The main purpose of the examination is to clarify possible causes of secondary osteoporosis.
The blood values also help the doctor plan the therapy: if, for example, the calcium level in the blood is very low, the patient must not be treated with certain osteoporosis medication.
Basic diagnosis of osteoporosis: who is it recommended for?
Basic diagnosis of osteoporosis should be carried out in all people with an increased risk of bone fractures. These risk groups generally include women and men over the age of 70.
An osteoporosis clarification is also recommended for people aged 50 and over who have a wide range of risk factors for osteoporosis-related fractures. These include, for example:
- Vertebral body fractures after minor injuries (such as falling from a standing position)
- hip fracture in mother or father
- Immobility, for example through being confined to bed for a long time or in a plaster cast after operations or accidents
- Underweight (body mass index below 20), weight loss, and anorexia (anorexia nervosa)
- Smoking and chronic obstructive pulmonary disease (COPD)
- high alcohol consumption
- hormone-related diseases such as Cushing's syndrome, hyperthyroidism, lack of growth hormone due to a dysfunction of the pituitary gland (pituitary gland), diabetes (diabetes mellitus type 1 and type 2)
- rheumatological diseases (rheumatoid arthritis, systemic lupus erythematosus, ankylosing spondylitis)
- Gastrointestinal disorders such as celiac disease, including gastric surgery (complete or partial removal of the stomach)
- neurological / psychiatric diseases such as epilepsy, schizophrenia, Alzheimer's, Parkinson's, stroke, depression
- Heart failure (heart failure)
- alcohol-related liver disease
- certain medications such as high-dose cortisone, anticonvulsants (anti-epileptics), antidepressants, glitazones (for type 2 diabetes), aromatase inhibitors (for breast cancer), anti-hormone treatment for prostate cancer, opioids (strong pain relievers)
Further investigations
In addition to the basic diagnosis of osteoporosis, the doctor can carry out further examinations in certain cases. Sometimes, for example, computed tomography (CT) or magnetic resonance imaging (MRI) is necessary to rule out other possible causes of the patient's symptoms. These imaging procedures can also be important for therapy planning, for example if a bone fracture must first be clarified more precisely.
In rare cases, the doctor will take a sample of the bone tissue (bone biopsy). It is examined more closely in the laboratory. This can be helpful, for example, if the other examinations have only produced unclear findings.
Osteoporosis: treatment
The osteoporosis therapy consists of several components. It is individually adapted to the patient. When planning therapy, the doctor takes into account, among other things, what triggered the bone loss and how pronounced it is.
General information on osteoporosis therapy
The most important basic measures of any osteoporosis therapy include sufficient exercise and proper nutrition. If necessary, the patient is given additional medication to combat bone loss.
Fall prevention is also important: osteoporosis patients break their bones easily. Here are some tips to reduce the risk of falls and accidents:
- The apartment should be adequately lit and furnished in such a way that it is not so easy to trip and fall. For example, remove tripping hazards such as sliding carpets and exposed cables.
- If the eyes are sagging, patients should wear suitable visual aids.
- High-heeled shoes and shoes with smooth soles are unsuitable. Flat shoes with non-slip soles are more advisable.
- If possible, osteoporosis patients should not take medication that restricts alertness and the ability to react. These include sleeping pills, allergy drugs and antidepressants.
In the case of secondary osteoporosis as a result of another disease (such as hyperthyroidism), this underlying disease must be treated. Otherwise the osteoporosis therapy might not bring the desired success.
If certain drugs have triggered secondary osteoporosis, one should switch to "more bone-friendly" preparations if possible - that is, drugs that have a less negative effect on bone density. This is recommended, for example, in women who are treated with glitazones for type 2 diabetes.
Movement as an osteoporosis therapy
With regular exercise, you can both prevent and treat bone loss. It is very important to choose the right form of exercise or sport.
First of all, there is no need for competitive sport for osteoporosis therapy! Efficient osteoporosis treatment starts with taking regular walks, for example. This promotes bone formation and inhibits bone breakdown. Light running training such as jogging or walking are also very effective.
Swimming is also recommended as a therapy for osteoporosis. Half an hour back or breaststroke swimming twice a week is ideal. Other muscle groups are also trained here than when walking, for example the back muscles.
Water aerobics and light weight training are also suitable for treating osteoporosis. You can do gymnastics outside the pool and simple osteoporosis exercises at home on your own. Here, too, you can achieve good effects with a half-hour training session twice a week. Tips for suitable exercises can be obtained from your doctor, sports medicine specialist or in a special sports group for osteoporosis patients, for example.
In general, the following applies: Discuss with your doctor which type of exercise and / or type of sport and which training intensity make the most sense in your case.
Diet as osteoporosis therapy
Every osteoporosis therapy includes - in addition to sufficient exercise - also the right diet. Here are the most important tips:
Eat a balanced diet. Make sure that you supply your body with sufficient calcium. The mineral is important for healthy, strong bones. Adults should add 1,000 milligrams of calcium to their bodies every day with their diet. It is mainly found in dairy products, but is also found in green vegetables such as spinach and broccoli and in some types of mineral water.Calcium is also added to some foods, such as juices.
Some patients cannot be certain that they are getting enough calcium from their diet. Then the doctor will also prescribe calcium supplements (e.g. effervescent tablets).
In addition to calcium, vitamin D is also very important for osteoporosis patients (and other people): It ensures that the body can absorb calcium from the intestines and build it into the bones. Good food sources of vitamin D are high-fat fish, eggs, butter, and milk.
In addition, you should regularly expose your skin to sunlight: With the help of UV light, the body can produce vitamin D itself. With this in-house production, he even covers most of his needs. In summer you should spend 5 to 15 minutes in the sun every day, in spring and autumn 10 to 25 minutes. It is sufficient to have the face and hands "irradiated". Depending on the temperature, you can let the sun act on your uncovered arms and legs.
Often, doctors also prescribe vitamin D supplements for osteoporosis. This is to ensure the supply. Such preparations are particularly useful for patients with a high risk of falling or broken bones who are not exposed to much sunlight. The daily dose is 800 to 1,000 international units (IU) of vitamin D3.
For solid bones, phosphate is also required, but in the right proportion to the calcium intake. An excess of phosphate binds calcium so that it can no longer be built into the bones. You should therefore avoid foods and drinks that are rich in phosphate, such as meat, sausage, processed cheese and cola drinks.
Phosphates can be recognized in the list of ingredients on food and beverage packaging by the numbers E 338-341 and E 450.
Medicines for osteoporosis
If osteoporosis patients are at high risk of fractures, the doctor will also prescribe drug therapy for osteoporosis. The following active ingredients are available:
- Bisphosphonates: Bisphosphonates such as alendronate and zoledronate are the first choice for osteoporosis therapy. They prevent excessive bone loss and strengthen the remaining bone mass. Bisphosphonates are taken in tablet form daily, weekly or monthly or given in the form of injections or infusions.
- Selective estrogen receptor modulators (SERM): The representative raloxifene from this group of active ingredients is approved for osteoporosis therapy. It binds to special docking sites (receptors) that are actually intended for estrogens, and thus inhibits bone breakdown. Raloxifene is taken daily as a tablet.
- Strontium ranelate: This active ingredient also inhibits bone breakdown and also increases the activity of the bone-building cells. It is taken daily as a powder solution.
- Teriparatide: Teriparatide is a derivative of the body's own hormone parathyroid hormone. It promotes bone formation and the formation of new bone structures. The active ingredient is injected under the skin once a day.
- Denosumab: Denosumab is a so-called monoclonal antibody. It intervenes in the bone metabolism and inhibits the bone-degrading cells (osteoclasts). Denosumab is given as an injection under the skin.
In individual cases, other drugs can be used for osteoporosis therapy, such as female sex hormones or calcitonin.
Pain therapy
The doctor can initiate suitable pain therapy for the pain associated with osteoporosis. Painkillers from the group of non-steroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen, acetylsalicylic acid (ASA) or diclofenac are often used. If the pain is severe, the doctor may also prescribe so-called opiates. In some cases, other medications such as muscle relaxants (muscle relaxants) are useful.
Physical therapy measures often help against osteoporosis pain. These include, for example, cold or heat treatments, massages or acupuncture. In some patients, the symptoms can be sufficiently alleviated. For others, physical therapies can complement pain reliever treatment.
In the event of persistent pain as a result of vertebral body fractures, the doctor can also prescribe a semi-elastic corset for the patient.
surgery
In the case of vertebral body ruptures, surgical intervention can be useful. In what is known as vertebroplasty, the surgeon applies bone cement to the broken vertebral body. This is stabilized as a result. In a kyphoplasty, the vertebral body is first expanded with a small balloon. This can straighten the bone a bit and also makes it easier to insert cement.
Other bone fractures due to osteoporosis also sometimes require surgery. For example, some patients receive an artificial hip joint after a femoral neck fracture.
More tips on osteoporosis therapy
- Avoid being underweight.
- Avoid nicotine and alcohol.
- Pay attention to back-friendly behavior in everyday life (for example an upright sitting position, regular change of sitting posture, no carrying heavy loads, no stooping posture when doing housework, replacing sagging mattresses).
It is also helpful to join a support group for osteoporosis patients. Such groups offer advice, help and exchange with other patients. Take advantage of this offer if you have the opportunity!
Osteoporosis: disease course and prognosis
Osteoporosis is currently not curable. It is all the more important to recognize and treat them as early as possible. Because without treatment, osteoporosis progresses further and further. Patients are increasingly suffering from bone pain (such as back or neck pain). The fractures accumulate. Especially in old age, many people find it difficult to recover from severe fractures.
The femoral neck fracture is particularly feared. It can lead to serious complications and secondary diseases such as rebleeding and wound healing disorders. The necessary operation (such as the use of an artificial hip joint) carries further risks for those affected. Many of the older patients are only able to move to a limited extent afterwards or even become nursing homes. About 10 to 20 percent of all patients with a femoral neck fracture die from secondary diseases or the risks of surgery.
Osteoporosis: prevention
Anyone who wants to prevent osteoporosis should minimize the known risk factors. These include, for example, a lack of exercise and a lack of calcium and vitamin D. Here are the most important tips:
- Eat a calcium-rich diet with dairy products and calcium-rich water. Adults should consume 1,000 to 1,500 milligrams of calcium per day.
- Eat foods that are high in vitamin D, such as high-fat fish (like herring), fish oil, and egg yolks on a regular basis.
- Expose your face and hands (and, if possible, other uncovered parts of the body) to sunlight regularly: five to 15 minutes a day in summer, ten to 25 minutes a day in spring and autumn. Then the body can cover a large part of its vitamin D needs by producing the vitamin itself.
- Avoid foods that are high in phosphate. They inhibit the absorption of calcium in the intestines and promote the release of calcium from the bones. Meat and sausage products, processed cheese and cola drinks, for example, are rich in phosphates.
- Refrain from tobacco and alcohol, and don't drink too much coffee. These luxury foods are also bad for the bones.
- Another essential component of osteoporosis prevention is regular exercise. Be physically active on a regular basis, preferably several times a week. That strengthens the bones.
Additional information
Guidelines:
- Guideline "Prophylaxis, Diagnosis and Therapy of Osteoporosis" of the umbrella organization of the German-speaking Scientific Osteological Societies e.V.
Self-help groups:
- Osteoporosis Self-Help Groups Dachverband e.V .: http://www.osd-ev.org/