Polyneuropathy
and Martina Feichter, medical editor and biologist Updated onDr. med. Julia Schwarz is a freelance writer in the medical department.
More about the expertsMartina Feichter studied biology with an elective subject pharmacy in Innsbruck and also immersed herself in the world of medicinal plants. From there it was not far to other medical topics that still captivate her to this day. She trained as a journalist at the Axel Springer Academy in Hamburg and has been working for since 2007 - first as an editor and since 2012 as a freelance writer.
More about the experts All content is checked by medical journalists.
In a polyneuropathy, peripheral nerves are damaged. These can be nerves in the arms and legs, for example, or those that supply internal organs. The most common causes of this nerve damage include diabetes mellitus and alcohol abuse. Read more about the symptoms, causes, diagnosis and treatment of polyneuropathy here.
ICD codes for this disease: ICD codes are internationally recognized codes for medical diagnoses. They can be found, for example, in doctor's letters or on certificates of incapacity for work. G63G61G62
Polyneuropathy: Brief Overview
- What is polyneuropathy? A group of disorders in which several or many peripheral nerves are damaged. These are the nerves outside the central nervous system (brain and spinal cord). The polyneuropathy is also called "peripheral polyneuropathy" or "peripheral neuropathy" (PNP).
- Symptoms: depending on which nerves are damaged. Often there are abnormal sensations, tingling, pain and numbness in the legs and / or arms, muscle weakness, muscle cramps and paralysis, bladder emptying disorders, constipation or diarrhea, impotence, cardiac arrhythmias, etc.
- Examinations: physical examination, electroneurography (ENG), electromyography (EMG), blood tests, etc.
- Causes: mainly diabetes and alcohol abuse. Other causes are other acquired diseases or poisoning. More rarely, polyneuropathy is genetic. Sometimes no cause can be found.
- Therapy: If possible, the cause is eliminated or treated. In addition, the symptoms can be treated in a targeted manner (for example with medication, TENS, physiotherapy, alternating baths, wraps, orthopedic aids).
Polyneuropathy: symptoms
In a polyneuropathy, peripheral nerves are damaged. These could be nerves that command muscle contractions (motor nerves) or control digestion or breathing (autonomic nerves). Nerves that are responsible for the sensitive perception of touch, temperature, pressure and vibration (sensitive nerves) are also often affected.
-
Polyneuropathy: diagnosis is detective work
Three questions for
Dr. med. Meike Maehle,
Specialist in neurology -
1
When should I go to the doctor with complaints?
Dr. med. Meike MaehleAt an early stage, if you notice that you have, for example, sensations in your feet or incoordination when walking. Then the family doctor and the neurologist with him can investigate the cause before the nerve is permanently damaged. In addition, nerves need time to recover - and therefore patience. Those who are treated early and well are more likely to become symptom-free again.
-
2
Who is particularly at risk?
Dr. med. Meike MaehleThere are people in whom the disease has a genetic cause. Those affected are then correspondingly younger. The symptomatic polyneuropathies, which are much more common, mainly affect older people. The nerve ailment is here, for example, a side effect of diabetes, vitamin deficiency diseases or alcohol addiction.
-
3
Can you quickly find the cause of polyneuropathies?
Dr. med. Meike MaehleUnfortunately not - it is often real detective work. Statistically speaking, you can only find a reason for the complaints in around 50 to 60 percent and can then often treat it directly. Nevertheless, there are some things that can be done without knowing the cause of the relief, for example physiotherapy or gait or walking training. Vitamin B complexes support the nerves in healing. And last but not least, there are also drugs that can relieve the pain.
-
Dr. med. Meike Maehle,
Specialist in neurologyDr. Maehle runs the Grünwald Neuropraxis in Munich, where she also treats polyneuropathies, among other things.

Which polyneuropathy symptoms occur in a patient therefore depends on the damaged nerves. Accordingly, a distinction is made between motor, autonomic and sensory disorders.
However, polyneuropathy symptoms can also be classified according to their distribution in the body:
- Most of the time, the symptoms of polyneuropathy affect both feet or both arms. This is called symmetrical polyneuropathy. If, on the other hand, the nerve damage only occurs on one side of the body, an asymmetrical polyneuropathy is present.
- If the nerve damage mainly affects areas of the body that are remote from the trunk (such as feet, hands), it is a distal polyneuropathy. Much less often, the disease extends to parts of the body near the trunk (proximal polyneuropathy).
Polyneuropathy Symptoms: Sensitive Nerves
Nerves that lead from the skin to the brain are called "sensitive". They inform the brain, for example, about touch, pressure, temperature or pain stimuli or vibrations. If this sensitivity is disturbed by a polyneuropathy, then the perception suffers, for example in the arms and legs. The toes are often the first to be affected. For example, there may be abnormal sensations, tingling or stabbing, burning pain.
Numbness is also a possible symptom of polyneuropathy. If these occur in the legs, those affected have coordination problems when walking, for example.
If the temperature sensation is disturbed, injuries can occur more easily. For example, polyneuropathy patients do not notice that their footbath is too hot. People with pronounced polyneuropathy can also only perceive pain to a reduced extent. This also increases the risk of injury.
Most polyneuropathies are associated with sensitive disorders.
Polyneuropathy Symptoms: Motor Nerves
Motor nerves carry commands from the brain to the skeletal muscles. The commands cause a muscle to contract (contract). In motor polyneuropathy, these nerves are damaged. As a result, the muscles in question lose strength. In the worst case, muscle paralysis occurs. Muscle cramps are also possible.
In general, if tissue is inadequately activated or not activated at all by the nerves supplying it for a long time, it degenerates - it shrinks and shrinks. This happens particularly quickly with the skeletal muscles. In severe cases, motor polyneuropathy can lead to muscle wasting (muscle atrophy).
Polyneuropathy Symptoms: Autonomic Nerves
The autonomic (vegetative) nerves control the function of internal organs such as the heart, lungs, stomach, intestines, genital organs and bladder. You are not subject to the will. For example, one cannot consciously order the heart muscle to contract.
Damage to autonomic nerves can lead to serious or even life-threatening symptoms. For example, if intestinal nerves are damaged in polyneuropathy, diarrhea or constipation can occur. If nerves that regulate bladder function are affected, urination, i.e. bladder emptying, is disturbed. Nerve damage in the lungs can cause respiratory failure. If the autonomic polyneuropathy affects nerves in the heart muscle, dangerous cardiac arrhythmias can result.
Overview of polyneuropathy symptoms
In the following table you will find important polyneuropathy symptoms at a glance:
|
Sensitive symptoms |
Motor symptoms |
Autonomous symptoms |
|
Tingling, pins and needles |
Muscle twitching |
Pupillary disorders |
|
Sting |
Muscle spasms |
Water retention (edema) |
|
Furry and numbness |
Muscle weakness |
Ulcers |
|
Feeling of being constricted |
muscular dystrophy |
decreased sweating |
|
Feelings of swelling |
Racing heart at rest | |
|
Feeling uncomfortable pressure |
Stomach paralysis (gastroparesis) | |
|
Feeling like walking on cotton wool |
Diarrhea, constipation | |
|
Unsteady gait (especially in the dark) |
disturbed emptying of the bladder | |
|
lack of temperature sensation |
Impotence (erectile dysfunction) | |
|
painless wounds |
Dizziness / fainting on standing up |
Diabetic polyneuropathy: symptoms
In the case of polyneuropathy as a result of diabetes (diabetes mellitus), the symptoms develop insidiously. The first thing that is usually damaged is the sensitive nerve fibers. Those affected then notice, for example, a feeling of numbness or tingling in the legs. Many also feel a burning pain in their feet ("burning feet syndrome").
These polyneuropathy symptoms are particularly noticeable at rest or at night. Some patients say they can barely stand the weight and touch of the duvet.
Often, diabetic polyneuropathy means that pain is only felt to a lesser extent. Then small injuries often go unnoticed. Because the blood circulation is disturbed in many cases of diabetes, this can result in poorly healing wounds. This usually happens on the feet (diabetic foot syndrome). The affected tissue can even die (necrosis). Most diabetics have polyneuropathy on both feet or legs.
In the further course, the polyneuropathy can spread to autonomic nerves. Possible consequences are, for example, difficulty swallowing, vomiting and alternating diarrhea and constipation. Urinary incontinence and erectile dysfunction (men) can also turn out to be symptoms of polyneuropathy.
Alcoholic polyneuropathy: symptoms
Alcoholic polyneuropathy is also widespread. It usually progresses slowly. Most people affected have nerve disorders in their legs, in both of them (symmetrical polyneuropathy): pain, abnormal sensations, sensory disorders, muscle wasting and severe muscle slackening (paresis) occur. Those affected can then no longer stand correctly, for example.
In severe cases, polyneuropathy symptoms also develop in the eye area, for example pupillary disorders and paralysis of the eye muscles
In some cases, alcoholic polyneuropathy has no symptoms.
Polyneuropathy: causes and risk factors
Doctors now know more than 200 different causes of polyneuropathy. The nerve damage is most often caused by diabetes (diabetic polyneuropathy) or alcohol (alcoholic polyneuropathy).
Polyneuropathy in diabetes
Diabetic polyneuropathy is the most common type of polyneuropathy. It can occur in both type 1 and type 2 diabetes.
It is estimated that one in two diabetics will develop polyneuropathy in their lifetime. The decisive factor here is whether and how well diabetes is treated: Diabetics whose blood sugar levels are poorly controlled develop polyneuropathy particularly early and particularly severely.
The mechanisms by which permanently high blood sugar damage the nerves has not yet been clarified in detail.
- On the one hand, the high levels of blood sugar can damage the nerves directly: Experts suspect that the sugar molecules form reactive compounds with various proteins. These attack the nerve cells and damage them irreversibly over time.
- On the other hand, the high blood sugar damages the tiny blood vessels in the body (microangiopathy). This can mean that nerves are no longer adequately supplied with oxygen and nutrients. Their function suffers as a result. Over time, the undersupplied nerves can even die.
Usually this nerve damage is insidious in diabetes patients. The symptoms of polyneuropathy appear slowly. The nerve damage is also different for each patient. The nature and severity of the symptoms can therefore vary considerably.
Polyneuropathy due to alcohol
The second most common cause of polyneuropathy is alcohol, namely chronic alcohol consumption. Here, too, the following applies: The exact mechanisms that lead to the nerve damage have not yet been fully clarified. However, research suggests that alcohol can attack nerves directly. This mechanism is believed to be primarily responsible for nerve damage in alcoholics.
A second factor may make things even more difficult: Alcoholism is often associated with malnutrition. Many alcoholics have a poor and one-sided diet. Among other things, this can lead to a deficiency in vitamin B12. However, this vitamin is very important for the functioning of the nervous system. A vitamin B12 deficiency could also promote nerve disorders in alcoholics. Because even on its own it can trigger polyneuropathy.
Other causes of polyneuropathy
Other possible causes of polyneuropathy include:
- Deficiency in vitamin B12 (for example in vegans or after gastric surgery)
- Kidney disease
- Liver disease
- Thyroid disorders (under and over function)
- gout
- Poisons (such as arsenic, lead) and drugs (especially cancer drugs)
- Solvents (e.g. hydrocarbons such as benzene or trichloroethene, alcohols such as methanol; therefore, toxic polyneuropathy is recognized as an occupational disease in certain professional groups such as painters or floor layers - after appropriate testing)
- certain infectious diseases such as Lyme borreliosis, diphtheria, Pfeiffer's glandular fever (mononucleosis), shingles, herpes simplex infections, HIV etc.)
- Guillain-Barré syndrome (an autoimmune disease)
- Fabry disease (a congenital metabolic disorder)
- Cancer (polyneuropathy may be the first sign here)
Most polyneuropathies are caused by such diseases or poisoning. Sometimes certain drugs that are used in cancer therapy, among other things, are the trigger. More rarely, nerve damage is genetically determined. There are various congenital diseases that are accompanied by polyneuropathy. This includes, for example, HMSN (hereditary motor-sensitive neuropathy), of which there are several sub-forms.
The cause of the polyneuropathy remains unexplained in around 20 percent of all patients.
If nerve toxins such as alcohol, heavy metals or drugs damage the nerves, it is a "toxic polyneuropathy".
Which part of the nerve cells is damaged?
Each nerve cell is made up of a cell body and a nerve process (axon). The axon can be up to a meter long. The nerve processes can be thought of as cables. The body protects its "nerve cables" with an insulating layer. This is known as the myelin layer or myelin sheath. In addition to its protective function, the myelin has another task: It accelerates the transmission of electrical nerve signals.
Depending on which part of a nerve cell is damaged, a distinction is made between demyelinating and axonal polyneuropathy:
Demyelinating polyneuropathy is characterized by the breakdown of the protective medullary layer (myelin layer). If, on the other hand, the axon itself is affected, it is an axonal polyneuropathy. Both forms can also occur in combination. Then myelin sheaths and axons are damaged equally.
Nerve damage in polyneuropathy
Polyneuropathy: examinations and diagnosis
If you notice any symptoms of polyneuropathy, you should consult a doctor immediately. If the nerve damage is recognized early and its cause treated, this has a positive effect on the course of the polyneuropathy.
Doctor-patient conversation
The doctor will first talk to you in detail to collect your medical history (anamnesis).He has the complaints described in detail and asks how long they have existed. He also asks about any previous or underlying diseases (such as diabetes, kidney diseases, underactive thyroid, etc.). Also, let the doctor know about any medications you are taking and any toxins you may be exposed to in the workplace.
Information on drug and alcohol consumption is also important for clarifying polyneuropathy. You should answer your doctor's questions openly and honestly. Only in this way can he find out the correct cause of the nerve disorders.
Examinations and tests
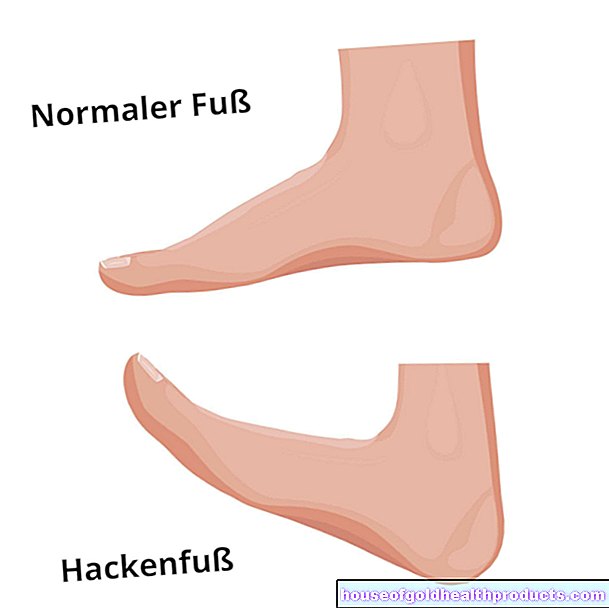
After the interview, the doctor will examine you physically. For example, he tests your reflexes (such as the Achilles tendon reflex, which is the first to weaken). It also checks whether your pupils respond correctly to incident light. The doctor also pays attention to possible malformations of the skeleton (deformities). For example, claw toes and arches foot can be an indication that the polyneuropathy is hereditary.
In addition, further investigations will follow. Some of these are done on every patient, others only in certain cases:
In electroneurography (ENG), the nerve conduction velocity is measured. To do this, the doctor applies a small electronic impulse to at least two different points on a nerve. Then he measures the time until the corresponding muscle reacts (contraction). In the case of polyneuropathy, this nerve conduction speed is usually reduced.
Electromyography (EMG) tests electrical muscle activity. In the case of motor disorders such as muscle weakness or muscle paralysis, it can be found out whether the problem is with the muscle itself or with the nerves supplying it. If the EMG shows that the nerve function is disturbed, this speaks for a polyneuropathy.
In the quantitative sensory examination, the doctor tests how a nerve reacts to certain stimuli such as pressure or temperature. In this way it can be determined whether the sensitivity of the nerve is impaired - as in a polyneuropathy. In this way, nerve damage can be proven well. However, the investigation is very time-consuming. In addition, the patient has to concentrate well and cooperate. Therefore, the method is not routinely used to clarify polyneuropathy.
Electrocardiography (EKG) can provide information about whether the heart's autonomic nerve fibers are damaged.
Using an ultrasound examination of the urinary bladder, the doctor can determine whether there is any residual urine in the bladder after urination. If so, your bladder emptying is likely to be disrupted. This happens very often with an autonomic polyneuropathy.
In a nerve biopsy, a tiny sample of nerve tissue is taken through a small incision in the skin. The tissue sample is then examined diagnostically under the microscope. However, this examination is only carried out in very specific cases. It may be necessary, for example, in diabetics in whom only nerves on one side of the body are damaged (asymmetrical diabetic polyneuropathy). Even if the doctor suspects leprosy as the cause of the nerve damage, they can perform a nerve biopsy.
A skin biopsy is also only performed in selected cases. A tiny piece of skin is punched out (on the lower leg, for example) and examined carefully.
Blood tests are primarily used to identify common and treatable causes of nerve damage. If there is a suspicion, rarer causes can also be uncovered on the basis of certain laboratory values. Some examples of laboratory tests for polyneuropathy are:
- Elevated inflammation levels (such as CRP, white blood cells etc.) can indicate an inflammatory cause of the nerve damage.
- An oral glucose tolerance test (oGTT) shows how well the body can process sugar. Abnormal test results can indicate undiscovered diabetes (or a precursor to it). The fasting blood sugar is also very meaningful here.
- In the case of known diabetes, the HbA1c value ("long-term blood sugar") is particularly important: It shows how well the diabetes has been controlled in the last few months.
- The vitamin B12 status is measured to check whether there is a possible deficiency.
- If the liver or kidney values are abnormal, the polyneuropathy may be caused by a liver or kidney disease. Liver damage can also be caused by alcohol abuse.
- If it is suspected that a certain infectious disease is causing the polyneuropathy, special blood tests are useful. For example, suspected Lyme disease can be clarified by looking for antibodies against the triggering bacteria (Borrelia) in the patient's blood.
Genetic testing is indicated when there are multiple cases of polyneuropathy in the family. Then the suspicion arises that it is a hereditary nerve damage.
The same applies if the patient has certain misalignments of the foot (claw toes, pesus) or other malformations of the skeleton (such as scoliosis). They are typical of hereditary polyneuropathy. The doctor can then have the patient's genetic material examined for corresponding changes (mutations).
Polyneuropathy: treatment
Effective polyneuropathy therapy includes eliminating or treating the cause of the disease - if possible. This is called causal therapy. Many polyneuropathy symptoms can also be specifically treated. This symptomatic therapy can complement causal therapy, if possible.
Causal therapy
Some examples of causal treatment for polyneuropathy are:
Alcoholics should go into withdrawal. In diabetic patients, the blood sugar must be adjusted correctly. If a vitamin B12 deficiency has been found, one should eat a more balanced diet and compensate for the deficiency with a vitamin supplement. If toxins or drugs are the trigger of the polyneuropathy, they must be avoided as far as possible.
In patients with a certain subgroup of polyneuropathies (chronic inflammatory demyelinating polyneuropathy), antibodies have been discovered that block the conduction of stimulus along myelinated fibers. Standard therapies respond poorly in these patients and those with immune-mediated neuropathy. However, treatment with rituximab - an artificially produced antibody that is used in cancer immunotherapy and in autoimmune diseases - has a good chance of success.
Symptomatic therapy
For example, the following symptomatic therapeutic measures are used:
Pain therapy
In many polyneuropathy patients, the nerve damage causes burning pain. These can be alleviated with pain therapy. The doctor often recommends pain relievers such as aspirin (acetylsalicylic acid) or paracetamol. He will select an individually suitable dosage for each patient.
For very severe nerve pain, he may also prescribe so-called opioids. These are very effective painkillers, but they have two disadvantages: On the one hand, their effect can wear off over time - in order to alleviate the pain, higher and higher doses are necessary. On the other hand, opioids can be addictive. Their use must therefore be carefully monitored by the doctor.
In the case of very persistent polyneuropathic pain, it can make sense for the patient to seek treatment from a pain therapist. He specializes in the therapy of chronic pain.
Anticonvulsants, such as gabapentin or pregabalin, can also help with nerve pain. They ensure that the nerve cells are less excitable. The nerve pain subsides as a result. The therapy with anticonvulsants is "crept in", that is: You start with a low dose, which is then slowly increased until the desired effect is achieved. This prevents side effects. In addition, the doctor will regularly examine the patient's blood during treatment. Antiepileptic drugs can change certain blood values.
As part of pain therapy, mood-enhancing agents (antidepressants) such as amitriptyline are often used. They inhibit the transmission of pain signals in the spinal cord. The pain is not taken away from the patient, but it becomes more bearable. As with the antidepressants, it is recommended to "sneak in" the therapy (initially low dose, then gradually increasing the dose). This lowers the risk of side effects such as a drop in blood pressure, irregular heartbeat or problems urinating.
Some polyneuropathy patients with nerve pain benefit from so-called TENS (transcutaneous electrical nerve stimulation), also known as electrical stimulation therapy. An electrode is placed on the painful area of the skin. It is connected to a small portable device. If necessary, the patient can deliver gentle electrical impulses to the skin area via the electrode at the push of a button. This can reduce the pain. How this is possible is not exactly known. But there are different theories. For example, some experts suspect that the electrical impulses release the body's own pain-relieving messenger substances (endorphins).
The effectiveness of TENS for nerve pain has not yet been scientifically proven.
Physical therapy
Physical therapies can help especially in the case of sensory and motor disorders of polyneuropathy. These include, for example, physiotherapy, contrast baths, electrical treatment of paralyzed muscles and warm and cold compresses. These procedures can, among other things, increase blood flow and strengthen weakened muscles. In addition, physical therapy helps polyneuropathy patients stay mobile despite pain and other limiting complaints.
Further therapeutic measures
Depending on the type and extent of the symptoms, other therapeutic measures may also be considered. Some examples:
For frequent calf cramps, polyneuropathy patients can try a gastric preparation. The active ingredient quinine may also help.
If polyneuropathy patients have great problems walking, orthopedic aids are useful. If, for example, the so-called peroneal nerve in the leg is damaged, those affected can hardly or no longer lift the foot. Then a special splint or a special shoe / boot will help.
If patients are plagued by a feeling of fullness, nausea and / or vomiting due to the polyneuropathy, it is advisable to change their eating habits: Several small dishes that are eaten throughout the day are better than a few large meals. In addition, nausea and vomiting can be relieved with prescription drugs (metoclopramide or domperidone).
If constipated, patients should drink a lot, eat a high-fiber diet, and exercise regularly. For acute diarrhea in polyneuropathy, the doctor can prescribe a drug (such as loperamide).
Autonomous disorders in polyneuropathies are, for example, circulatory problems when getting up from lying down or sitting (orthostatic hypotension): The affected person becomes dizzy or even faints due to a sudden drop in blood pressure. As a preventive measure, patients should always stand up slowly. Support stockings can also help: They prevent the blood from sinking into the legs when you stand up and thus triggering circulatory problems. Regular muscle training is also useful. If necessary, the doctor can also prescribe medication for low blood pressure.
If polyneuropathies cause bladder weakness, patients should go to the toilet regularly (for example every three hours) - even when there is no urge to urinate. Then too much residual urine cannot collect in the bladder. That is because it favors a bladder infection.
Impotence (erectile dysfunction) can result from the polyneuropathy itself as well as from drugs such as antidepressants. In the second case, patients should discuss with their doctor whether the medication can possibly be discontinued. If this is not possible or the impotence persists afterwards, affected men can make do with a vacuum pump. The doctor may also be able to prescribe a sexual enhancer (Sildenafil, etc.).
Polyneuropathy: course and prognosis
The course of the polyneuropathy can be positively influenced by eliminating or treating the trigger (if possible). The symptoms can also be alleviated with various therapies. Nevertheless, many patients ask themselves: can polyneuropathy be cured?
Basically, the earlier the nerve damage is recognized and treated, the better the prognosis. Unfortunately, the polyneuropathy often has no symptoms for a long time or the first slight complaints are not taken seriously. At the time of diagnosis, the disease is already well advanced. Often there is already irreversible nerve damage from the polyneuropathy. Healing is then no longer completely possible. With the right treatment, however, one can try to prevent further nerve damage from polyneuropathy and to improve existing symptoms.
Additional information:
Books:
- How to treat polyneuropathy - holistically and effectively: The first guide for those affected by laymen (Sigrid Nesterenko, 3rd edition 2019, Rainer Bloch Verlag)
- Polyneuropathy: How to overcome excruciating nerve pain (Udo Zifko, 2019, Springer-Verlag)
- Guide to polyneuropathy and restless legs: Living with numb feet, painful and restless legs (Christian Schmincke, 2021, Springer-Verlag)
Guidelines:
- Guideline "Diagnostics in polyneuropathies" of the German Society for Neurology (status: 2019)
Tags: magazine parasites travel medicine

.jpg)