Dysarthria
and Sabine Schrör, medical journalistMartina Feichter studied biology with an elective subject pharmacy in Innsbruck and also immersed herself in the world of medicinal plants. From there it was not far to other medical topics that still captivate her to this day. She trained as a journalist at the Axel Springer Academy in Hamburg and has been working for since 2007 - first as an editor and since 2012 as a freelance writer.
More about the experts
Sabine Schrör is a freelance writer for the medical team. She studied business administration and public relations in Cologne. As a freelance editor, she has been at home in a wide variety of industries for more than 15 years. Health is one of her favorite subjects.
More about the experts All content is checked by medical journalists.Dysarthria is a neurological speech disorder. It can affect breathing, sound formation, pitch, speech rhythm and articulation. Speech comprehension does not suffer - unlike aphasia, dysarthria patients have no problems with sentence structure, word finding or reading and writing. Common causes of dysarthria are inflammatory processes in the brain, traumatic brain injuries, strokes or degenerative diseases such as Parkinson's. Read more about the origins, causes, forms and treatment options of dysarthria here.

Brief overview
- What is dysarthria? Neurologically caused speech disorder as a result of damaged nerve and / or muscle structures responsible for speech motor skills. Differentiation from aphasia as a language disorder with limited understanding and processing of language as well as problems with finding words and sentence structure, for example.
- Causes: e.g. stroke, traumatic brain injury, early childhood brain damage, inflammation of the brain (encephalitis), meningitis (meningitis), brain tumor, multiple sclerosis, Parkinson's disease, amyotrophic lateral sclerosis, Huntington's disease
- Forms: spastic (hypertonic) dysarthria, hypotonic dysarthria, hyperkinetic dysarthria, hypokinetic (-rigid) dysarthria, atactic dysarthria, mixed dysarthria
- Diagnostics: anamnesis, neurological examinations, possibly electroencephalography (EEG), computed tomography (CT), magnetic resonance imaging (magnetic resonance imaging, MRT), liquor diagnostics (examination of the spinal fluid)
- Treatment: Treatment of the underlying disease, individual speech therapy, possibly aids such as soft palate prosthesis, electronic voice amplifier
Dysarthria: description and development
Speech motor skills are impaired in dysarthria. Those affected know exactly what and how they want to say something. But the nerve and muscle structures responsible for speaking cannot correctly execute the corresponding commands from the cerebral cortex.
This happens when the nerve and / or muscle structures responsible for speech motor skills have been damaged due to a stroke, meningitis, Parkinson's disease or alcohol abuse. Those affected then also have problems chewing and swallowing. In addition, their facial expressions are restricted.
Dysarthria can vary in severity. It affects the sound formation most clearly. In addition, the speed of speech, speech melody, speech breathing and voice training are usually also changed. The most severe form of dysarthria, in which those affected can no longer articulate themselves, is called anarthria.
Difference to language disorder
Speech disorders (dysarthria) are to be distinguished from speech disorders (aphasia): With these, those affected can no longer understand and process language correctly. They also have problems finding the right words and forming correct, meaningful sentences. In the case of dysarthrias, however, these higher brain functions are not impaired.
Dysarthria: causes
The causes of dysarthria are many. The most common are:
- Stroke (apoplexy): In the event of a stroke, the brain is suddenly no longer supplied with enough blood and thus oxygen. Usually a blood vessel occlusion caused by a clot is behind it, more rarely a cerebral haemorrhage. Strokes very often cause speech disorders. Stroke patients often also develop aphasia.
- Traumatic brain injury (TBI): The term traumatic brain injury summarizes all closed and open skull injuries with brain involvement that result from the impact of force on the head (for example from a blow or fall). This can result, among other things, in speech disorders (aphasia) and speech disorders.
- Early childhood brain damage: If the child's brain is damaged between the sixth month of pregnancy and the end of the first year of life, this can also lead to dysarthria.
- Inflammation of the brain (encephalitis): Viruses usually trigger an infectious inflammation of the brain, rarely bacteria. Dysarthria is one of the possible symptoms of encephalitis.
- Inflammation of the meninges (meningitis): Inflammation of the meninges caused by bacteria or viruses can also cause dysarthria.
- Brain tumor: Depending on the location, brain tumors can trigger different forms of dysarthria.
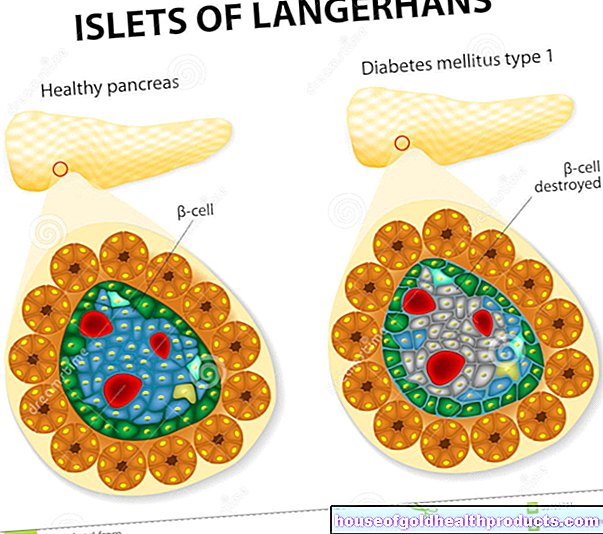
- Multiple sclerosis (MS): In this chronic inflammatory disease of the nervous system (spinal cord and brain), the immune system destroys the protective layer around the nerve fibers (myelin sheaths) so that nerve impulses can no longer be transmitted without interference. Among other things, this can lead to dysarthria.
- Parkinson's disease: Parkinson's disease is one of the most common diseases of the nervous system and is colloquially known as paralysis. Around 90 percent of all Parkinson's patients develop dysarthria.
- Amyotrophic lateral sclerosis (ALS): This rare chronic disease of the nervous system impairs motor skills, breathing, communication and food intake. Speech disorder can be an early symptom of ALS.
- Huntington's disease: In adults with hyperkinetic dysarthria, the cause is usually Huntington's disease - a rare hereditary disease that is associated with sudden, involuntary, irregular movements, among other things.
- Myasthenia gravis: In this rare autoimmune disease, the transmission of stimuli between nerve and muscle cells is disturbed. This can lead to dysarthria, among other things.
- Poisoning (intoxication): Poisoning, for example through alcohol abuse or drug consumption, is also one of the possible causes of dysarthria.
Dysarthria: forms
Doctors distinguish six forms of dysarthria:
- Spastic (hypertonic) dysarthria: Characteristic is increased muscle tension (hypertension) of the speech muscles, which can therefore only be moved to a limited extent. This affects breathing, voice training, and articulation. A compressed, rough voice is typical. In addition, those affected can only articulate themselves intermittently and indistinctly.
- Hypotonic dysarthria: In contrast to spastic dysarthria, muscle tension is reduced in hypotonic speech disorder - the muscles are limp and weak. Those affected tire quickly when speaking and can only articulate indistinctly. In addition, the volume and speech melody can be changed.
- Hyperkinetic dysarthria: Typical of this are exaggerated, explosive speech movements. Volume, pitch, and articulation vary widely. Sometimes those affected involuntarily grimace, wiggle or click their tongue.
- Hypokinetic (-rigid) dysarthria: Here the muscles of the breathing, larynx, tongue and face have only limited mobility. As a result, breathing is shortened, the speaking volume and the pitch range are restricted. Those affected speak in a monotonous voice and articulate themselves indistinctly. Mimic skills can also be severely impaired.
- Atactic dysarthria: People with atactic dysarthria speak very unevenly, that is, volume, pitch and the accuracy of the articulation vary greatly; all speaking is characterized by involuntary, inappropriate changes in breathing, voice, and articulation.
- Mixed dysarthria: In many cases, dysarthria cannot be clearly assigned to one of the groups mentioned. Because often several areas of the brain are damaged, so that those affected show, for example, both atactic and spastic dysarthria symptoms.
Dysarthria: When Should You See a Doctor?
Speech disorders should always be checked by a doctor - regardless of whether they develop slowly (as in Parkinson's or multiple sclerosis) or suddenly (as in a stroke or traumatic brain injury).
Dysarthria: what does the doctor do?
If dysarthria occurs suddenly as a result of a stroke or traumatic brain injury, the cause is clear. The primary focus here is on initial medical care for the patient.
Otherwise, the diagnosis starts with a detailed doctor-patient discussion about the medical history (anamnesis). If necessary, relatives are included in the conversation. The doctor asks, for example, when the speech disorder first appeared, how often it is noticeable, which complaints are in the foreground and what the general performance of the patient is like.
This is followed by a neurological examination with the aim of determining the disease underlying the dysarthria and the exact location of the brain damage.
Further examinations are possible, for example the measurement of electrical brain activity (EEG), imaging methods such as computed tomography (CT) and magnetic resonance imaging (MRT) as well as the removal and analysis of a sample of the cerebrospinal fluid (liquor diagnostics).
In a speech therapy examination, articulation, voice formation (phonation) and breathing are checked. This is important for therapy planning (speech therapy).
Dysarthria: which therapies help?
First of all, of course, the underlying disease that led to dysarthria (such as stroke, encephalitis, Parkinson's) must be treated.
The dysarthria itself is primarily treated with speech therapy. The most important goal is to maintain or restore the patient's independent communication skills.
Since there are different forms of dysarthria and the speech disorder can also develop differently, each speech therapy is individually adapted to the needs and resilience of the patient. Daily sessions as well as weekly or monthly therapy sessions are possible, individually or in a group.
Building blocks of speech therapy
In speech therapy, patients learn how to speak more intelligibly with a conscious head and body posture. The therapist uses special exercises to promote the harmonious interplay of breathing, voice and articulation. If the body tension is too high (spastic dysarthria), relaxation exercises help, if the body tension is too low (hypotonic dysarthria), tension-building training units are useful.
If breathing is impaired, breathing deepening and breathing flow lengthening are practiced, with particular emphasis on abdominal breathing. Voice exercises train the larynx muscles, various passive and active exercises train articulation. Concrete speaking exercises (sounds, words, sentences and texts) encourage spontaneous speaking and communication in everyday life.
Affected people who have particular problems speaking in certain situations can discuss this with the therapist. Dealing with such critical situations can then be practiced in role play, for example.
In very severe cases of dysarthria, the patient works with the therapist to develop alternative forms of communication. Instead of speaking, facial expressions, gestures and written language can also be used to make yourself understood.
Communication aids
In certain cases, special communication aids can be useful. Patients whose soft palate has limited mobility (velum insufficiency) can benefit from a soft palate prosthesis.
Electronic amplifiers can amplify the voice of very low-volume dysarthria patients. Alternative communication systems such as portable electronic typewriters are intended for dysarthria patients who can barely articulate themselves or can no longer speak intelligibly (for example in the late stages of amyotrophic lateral sclerosis).
Coping with illness
People with dysarthria can no longer express themselves easily. Many feel helpless and therefore react angry, aggressive, sad or develop depression. Some withdraw completely and avoid social contacts. Discussions in which therapists advise those affected and their relatives on how to deal with the dysarthria and the underlying disease can help. In severe psychological crises, psychological help is indicated.
Dysarthria: You can do that yourself
Both dysarthria patients and their interlocutors can contribute a lot to successful communication. Important points are:
- Avoid stress and excitement: Conversations should be conducted without hectic and in a quiet environment. Both sides - dysarthria patient and interlocutor - should take time to speak and understand. Noise sources in the immediate vicinity (radio, TV, machines, ...) should be avoided or switched off.
- Seek proximity: Conversations with dysarthria patients should be conducted as close as possible. This prevents the patient from having to exert himself excessively, which can impair intelligibility.
- Maintain eye contact: During the conversation, the dysarthria patient and the person opposite should keep eye contact. This is because the patient can make himself understood more easily through supporting facial expressions and gestures.
- Asking: If you haven't understood a dysarthria patient, don't be afraid to ask. Critical comments ("Speak more clearly!" Or "Speak louder!") Should be avoided!
- Do not speak for the person affected: In larger discussion groups one should not speak for a person with dysarthria, so do not relieve him of the sometimes difficult communication! This is usually well meant, but ultimately only harms the person concerned because he is excluded from the conversation.
- Show respect: a speech disorder is not a mental handicap. People with dysarthria should never be made to feel as if they are mentally disadvantaged or underage.







.jpg)








.jpg)