dizziness
and Sabine Schrör, medical journalist and Carola Felchner, science journalistSabine Schrör is a freelance writer for the medical team. She studied business administration and public relations in Cologne. As a freelance editor, she has been at home in a wide variety of industries for more than 15 years. Health is one of her favorite subjects.
More about the expertsCarola Felchner is a freelance writer in the medical department and a certified training and nutrition advisor. She worked for various specialist magazines and online portals before becoming a freelance journalist in 2015. Before starting her internship, she studied translation and interpreting in Kempten and Munich.
More about the experts All content is checked by medical journalists.Dizziness (vertigo) occurs relatively often. It is estimated that almost every third person will experience a moderate to severe attack of dizziness at some point in their life, with the incidence increasing with age. The dizziness is mostly temporary, but there is also permanent dizziness. The causes are mostly harmless. However, dizziness can also indicate a serious illness. Read more about the causes and treatment of dizziness here!

Brief overview
- Description: Vertigo can appear in various forms (e.g. as vertigo or vertigo), once or repeatedly. The cause is usually harmless, but sometimes a serious illness.
- Causes: e.g. small crystals in the equilibrium organ, nerve inflammation, Menière's disease, migraine, epilepsy, impaired cerebral circulation, motion sickness, cardiac arrhythmias, heart failure, hypoglycaemia, medication, alcohol, drugs
- Dizziness in old age: not uncommon; can have various causes, but also remain unexplained.
- When to the doctor If dizziness occurs suddenly, intensely and repeatedly without an apparent cause or during an infection, is triggered by certain situations or head postures, or is accompanied by other symptoms (nausea, vomiting, headache, visual disturbances, etc.). Always have dizziness clarified in old age.
- Diagnostics: including taking the medical history, physical examinations, further examinations as required (such as neurological examination, long-term blood pressure measurement, imaging, EEG, blood tests)
- Therapy: depending on the cause, e.g. medication, regular positioning maneuvers of the head, behavior therapy, aids such as walking stick or walker
- What you can do yourself: among other things, sleep and drink enough, eat regularly, reduce stress, avoid alcohol and nicotine, regularly measure blood pressure and, in the case of diabetes, blood sugar, special exercises
What is dizziness?
Along with headache and back pain, dizziness is the most common symptom in the nervous system. The likelihood of a dizziness attack increases with age: At a young age, severe dizziness only occurs in one in six to tenth people. In contrast, more than 30 percent of those over the age of 75 are affected.
For example, small children, i.e. children under two years of age, are almost "immune" to dizziness. Their sense of balance is still poorly developed. In the first few years of their lives, driving on winding roads or staying on a swaying boat can therefore do little to harm them. In older children, on the other hand, dizziness is a relatively common phenomenon, for example when they have eaten or drank too little. Adolescents after puberty are then often less prone to problems with balance.
The sense of balance
Three sensory organs work together to enable spatial orientation and control the sense of balance:
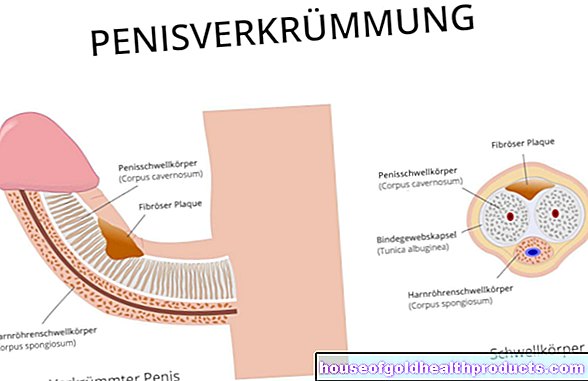
The vestibular apparatus is located between the eardrum and the cochlea in the inner ear. The fluid-filled cavity system consists of three semicircular canals (an upper, a lateral and a posterior), two atrial sacs and the endolymphatic duct (ductus endolymphaticus). When the body rotates or accelerates (e.g. on the carousel, when driving a car), the fluid in the vestibular apparatus moves, which irritates the sensory cells on its walls. The balance nerve (vestibular nerve) transmits these stimuli to the brain.
There are also stimuli of the eyes that provide information on how spatial fixed points and the horizon move.
Deep receptors in muscles, tendons and joints are the third element of the sense of balance. These tell the brain, for example, when the knee joint has to compensate for fluctuations.
The organs of equilibrium

Dizziness in old age - a special case?
As people get older, they are more likely to suffer from dizziness. Around every fourth person over 60 reports occasional attacks of dizziness. In fact, every second person over the age of 75 is affected. The fact that dizziness increases with age is due, among other things, to age-related changes and age-typical diseases. The latter can have dizziness as a symptom themselves or are treated with medication that causes dizziness as a side effect. If no specific cause can be found for the dizziness in older people (such as cardiovascular disease, visual disturbances, medication), doctors speak of dizziness in old age.
Dizziness often manifests itself in old age as a "wobbly" gait. This unsteady gait in older people can have dire consequences: Seniors can no longer react as quickly and are therefore often poorly able to cope with a fall. In addition, physical resistance decreases with age, which is why injuries are more likely to occur. For example, dizziness as a result of imbalance in the elderly can quickly lead to broken bones or other serious injuries.
Dizziness: causes
Dizziness often occurs when the brain receives contradicting information from the aforementioned sensory organs. Alternatively, dizziness can occur when the brain cannot properly process the incoming signals. In addition, physical and mental illnesses can be responsible for attacks of dizziness. So there are many causes of dizziness. In principle, doctors differentiate between vestibular and non-vestibular vertigo. The dizziness in old age can have both vestibular and non-vestibular causes ..
Vestibular dizziness
Vestibular dizziness occurs "in the head" - either through contradicting stimuli or a disturbed processing of the information that is passed from the balance organs to the brain. The trigger for this are illnesses or irritations of the equilibrium system.
Those affected usually experience the vertigo attacks as vertigo. If the inner ear or the equilibrium nerve is affected, it is a peripheral vestibular vertigo. In diseases of the brain stem, cerebellum or cerebrum, one speaks of central vestibular vertigo.
The most common forms and causes of vestibular dizziness are:
Benign paroxysmal positional vertigo (BPPV)
The harmless positional vertigo is the most common form of vertigo. It is triggered by the smallest crystals or stones (otoliths) in the fluid-filled equilibrium organ (cupulolithiasis, canalolithiasis). If the person concerned changes their posture, the stones or crystals move in the semicircular canals and thus irritate the sensory cells on the walls. An acute, short and violent attack of dizziness is the result, which can also occur when lying down. Nausea can also occur. However, hearing impairment is not one of the side effects.
Vestibular neuritis
Inflammation of the equilibrium nerve is the second leading cause of peripheral vestibular dizziness. It is not yet known why the nerve becomes inflamed. The inflammation triggers an extremely uncomfortable, persistent vertigo. Symptoms will only slowly resolve over the course of two to four weeks. Occasionally, shorter vertigo attacks announce the main attack a few days in advance.
Vestibulopathy
Spinning or staggering vertigo is typical of this inner ear disease. Those affected can only perceive their surroundings in a blurred manner, can no longer read street signs or can no longer reliably recognize the faces of people oncoming. The symptoms can last between a few minutes and a few days and are usually worse in the dark and on uneven ground.
For example, vestibulopathy can be caused by drugs that damage the inner ear (such as certain antibiotics such as gentamicin). Menière's disease (see below) and meningitis (meningitis) are also possible triggers.
Vestibular paroxysmia
Here, vertigo attacks (mostly vertigo, more rarely vertigo) occur regularly, which last only seconds to minutes and lead to unsteady standing and walking. Certain head positions can trigger the seizures. The causes of vestibular paroxysmia are unclear. It is believed that there is a kind of short circuit between two neighboring nerve fibers (axons).
Meniere's disease
Typical of Menière's disease are regularly occurring, sudden vertigo, one-sided tinnitus and one-sided hearing loss. The dizziness is not permanent, but occurs like attacks. An attack can last between 20 minutes and 24 hours. Menière's disease usually occurs between the 40th and 60th year of life noticeable, rarely in childhood.
Basilar migraines (vestibular migraines)
This particular form of migraine is associated with recurring attacks of dizziness. These are accompanied by visual disturbances, stance and gait disturbances as well as pain in the back of the head.
Circulatory disorders in the brain
Dizziness can also occur when the brain is no longer supplied with sufficient blood. This happens, for example, in the event of a stroke or a transitory ischemic attack (TIA) - a temporary circulatory disorder in the brain that is an early warning sign of a stroke! Other typical symptoms of dizziness as a result of disturbed cerebral hemorrhage are nausea and vomiting, disturbed movement sequences (ataxia), sensory disturbances, swallowing disturbances and speech motor disorders (dysarthria).
Acoustic neuroma
This benign tumor of the auditory and equilibrium nerves (eighth cranial nerve) originates from the Schwann cells that surround the nerve. As soon as the tumor reaches a certain size, it can trigger symptoms such as hearing loss, dizziness (vertigo or vertigo) and nausea.
Temporal bone fracture with labyrinth failure
In the event of a serious accident or fall, skull bones can break (skull fracture). If the petrous bone is affected (the section of bone that surrounds the inner ear), the inner ear with its equilibrium system can also be damaged. Dizziness is one of the possible consequences.
Vestibular epilepsy
Vestibular epilepsy is characterized by seizures with dizziness and rapid, twitching eye movements (nystagmus). Dizziness is often the first symptom and precedes the actual attack.
Motion sickness (kinetosis)
Unusual movements (for example when driving a car or bus on winding roads, turbulence in the plane or strong waves) can flood the inner ear with stimuli. If the person concerned does not constantly follow the causes of these movements with their eyes, the brain cannot assign the stimuli and registers them as an error message. This can happen, for example, if someone does not look at the road while driving, but at a map. For the brain, the person concerned then sits still - the card does not move as the eyes register. But the other organs of equilibrium report fluctuations and vibrations in locomotion to the brain. Dizziness, nausea, headaches and vomiting are often the consequences.
Non-vestibular vertigo
Anyone who suffers from non-vestibular dizziness can no longer orientate themselves in space, walks and stands unsteadily and therefore tends to fall. However, nausea and vomiting are rare with this type of dizziness.
In non-vestibular vertigo, the organs of equilibrium function properly. The nerves and brain are also completely intact. Rather, the triggers are found in other parts of the body. The causes of non-vestibular vertigo therefore include:
- Cervical spine syndrome (cervical spine syndrome): This complex of symptoms includes various complaints such as neck, shoulder and headache, often with neurological symptoms such as tingling or numbness in the fingers. Dizziness and tinnitus can also occur. Possible causes are signs of wear and tear, muscle tension, inflammation and injuries in the cervical spine area.
- Low blood pressure (hypotension) and orthostatic dysregulation: The latter means a sudden drop in blood pressure after changing position, e.g. when getting up quickly from lying down. The blood sags into the legs, causing the brain to briefly receive too little blood and thus too little oxygen. The consequences are dizziness and blackness in front of the eyes.
- High blood pressure (hypertension)
- Anemia
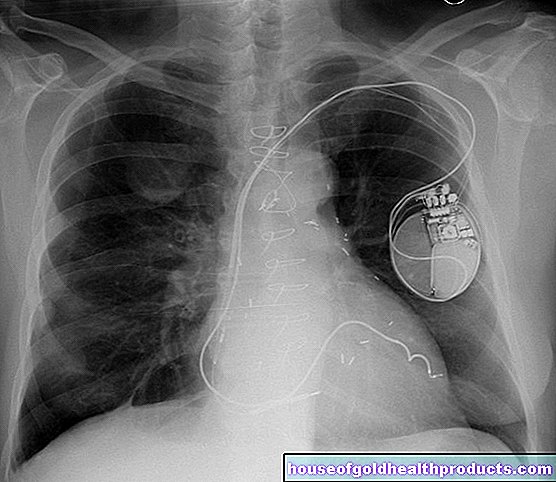
- Cardiac arrhythmias
- Heart failure (heart failure)
- Pulmonary embolism (a rare cause of dizziness)
- Pregnancy: The severe physical changes during pregnancy can be associated with fluctuations in blood pressure, which sometimes make you feel dizzy.
- low blood sugar level (hypoglycaemia)
- Vegetative diabetic polyneuropathy: Diabetes-related nerve damage in the area of the autonomic nervous system
- Vascular calcification and narrowing (arteriosclerosis) in the area of the vessels supplying the brain
- Carotid sinus syndrome: Certain pressure receptors in the carotid artery react overly sensitively - even with slight pressure they slow the heartbeat. This lowers blood pressure, which can cause dizziness and impaired consciousness (up to and including fainting).
- Medication (dizziness as a side effect)
- Alcohol and other drugs
- Hyperventilation: excessively fast and deep breathing
- badly adjusted or unfamiliar glasses
Dizziness often develops without a recognizable physical cause (somatoform dizziness). Those affected then suffer from various complaints, from dizziness to shortness of breath to listlessness. These symptoms are mostly due to mental illness such as an anxiety disorder or depression.
Phobic postural vertigo is the most common somatoform vertigo disorder. In the 30 to 50 age group, it is the most common type of vertigo. Drowsiness, vertigo, stance and gait insecurity as well as frequent falls are typical. The dizziness attacks occur when the person concerned is confronted with typical triggers of panic attacks, for example when crossing a bridge or in the middle of a crowd. The phobic vertigo is a psychogenic vertigo, that is, psychologically conditioned.
Causes of dizziness in old age
Dizziness in old age can be triggered by a variety of factors. Often it is benign positional vertigo (benign paroxysmal positional vertigo, see above) - ear stones in the inner ear that slip when moving and thus "confuse" the brain.
Age-typical diseases such as high or low blood pressure, vascular diseases, Parkinson's, metabolic disorders or diabetes mellitus (diabetes) can cause dizziness in older people. The same applies to some medications that are often taken by the elderly (e.g. blood pressure medication).
Often, however, dizziness in old age is simply a result of the aging process. Because the sensory organs, which are necessary for us to be able to move without giddiness, get older and then no longer function optimally.
The inner ear is sometimes poorly supplied with blood, nerve transmission slows down, and stimulus processing in the brain deteriorates. This can manifest itself in staggering and spinning vertigo or drowsiness and the associated balance disorders in old age. The eyes, which decline with age and limit spatial vision, can also contribute to this. In addition, decreasing muscle mass and strength can interfere with depth and surface perception, which can also cause or intensify feelings of dizziness.
Another factor that may not be obvious, but which is all the more important, are emotional reasons. According to the German Seniors League, depression, loneliness, grief and the like account for around a third of all vertigo cases in old age.
If you are accompanied by symptoms such as paralysis, visual disturbances, vomiting, sudden hearing loss or headache, you should contact a doctor immediately. It could be a serious cause like a stroke!
Dizziness: symptoms
A distinction is made between vertigo, vertigo, lift vertigo and pseudo-vertigo.
- Vertigo: The environment seems to revolve around the person concerned. This typically happens after excessive alcohol consumption. Vertigo can also have many other causes (e.g. suddenly getting up from lying down). It is often accompanied by nausea, vomiting, ringing in the ears and impaired hearing.
- Vertigo: those affected have the feeling that the ground is being pulled from under their feet. This is how vertigo can lead to an unsteady gait. People even feel dizzy when they stand still. Concomitant symptoms are very rare.
- Lift dizziness: People think they are falling and feel as if they are going up or down quickly in an elevator.
- Pseudo-vertigo: Here those affected feel drowsy and go black before their eyes - without the environment appearing to be moving. That is why one does not speak of "real" here, but of pseudo-fraud.
Dizziness: when do you need to see a doctor?
An acute attack of dizziness is often caused by a harmless positional dizziness that usually subsides on its own (spontaneously) within days or weeks. However, if you suspect that it is a different form of dizziness or if the dizzy spells keep recurring, you should consult a doctor. This is especially true when
- the dizziness occurs suddenly, violently and repeatedly without any apparent cause
- certain head movements always lead to dizziness,
- Nausea, vomiting, headache, ringing in the ears, drowsiness, visual disturbances or shortness of breath accompany the dizziness,
- the dizziness occurs during an infection with or without a fever or
- the imbalance occurs again and again in certain situations, for example in crowds or when driving a car. A visit to a doctor is also recommended if you suffer from dizziness caused by stress.
Many sufferers dismiss dizziness in old age as a side effect of the aging process that has to be accepted or simply played down. In doing so, it should be taken seriously and clarified by a doctor. It may be due to an illness that requires treatment. In addition, it is important to prevent the elderly affected from withdrawing and hardly leaving the house for fear of dizziness and possible falls.
Dizziness: what does the doctor do?
The causes of dizziness affect different medical specialties. Patients therefore often have to visit various specialists (such as ENT doctor, internist, neurologist) to determine the cause of their dizziness. In many cities today there are vertigo clinics in which specialists from various fields work together. If there is such an ambulance in your area, you should be examined and advised there. Otherwise, you can turn to your family doctor as the first point of contact.
Medical history and physical examination
First, the doctor will ask you about your medical history (anamnesis). Possible questions are:
- How does the dizziness feel (turning, swaying, moving up and down)?
- Do you go black or do you see asterisks?
- Is the dizziness more or less permanent or does it occur like a seizure?
- For dizziness attacks: how long do they last?
- Are there certain situations in which you feel dizzy (e.g. when turning, when getting up, in the dark)?
- Is the dizziness accompanied by other complaints (such as nausea, sweating, palpitations)?
- What are your lifestyle habits (diet, physical activity, sleep ...)?
- Do you suffer from any underlying illnesses (e.g. diabetes, heart failure)?
- Do you take any medicine?
It can also be helpful to keep a vertigo diary as a victim. There you write down when and in what form you became dizzy. The detailed information helps the doctor to find the cause.
In most cases, the anamnesis already provides information about the underlying type of dizziness. A physical exam will provide more information. For example, the doctor measures your pulse and blood pressure. If the pulse is irregular, he can create an electrocardiogram (EKG), for example to detect cardiac arrhythmias. A pregnancy test may also be required for women.
Sometimes further examinations are needed to clarify the cause of the dizziness:
Nystagmus examination
Nystagmus is an uncontrollable, rhythmic movement of the eyes ("eye tremors"). It is used to keep the image projected through the eye lens constant on the retina, i.e. to compensate for movements. In dizziness patients, however, this eye movement also occurs at rest. It can be observed with special glasses (Frenzel glasses).
Sometimes the doctor also provokes the nystagmus by, for example, turning the patient on a swivel chair or performing a warm ear irrigation, which irritates the organ of equilibrium in the inner ear.
Balance check
With the help of various balance and coordination tests, the medical professional can determine how well the balance system is working. In the Romberg test, for example, the patient has to stand still for at least one minute with arms outstretched forwards, feet closed and eyes initially open and then closed.
The doctor can also check the gait pattern for fluctuations or crooked walking.
In the Unterberger step attempt, the person concerned steps on the spot with closed eyes. A patient with disturbed nerve reflexes rotates around his own axis.
Hearing test
The doctor usually also examines the hearing ability in patients with dizziness, since hearing and sense of balance use the same nerve pathways. The examination is often carried out using a Weber test. The doctor holds a vibrating tuning fork to the patient's head and asks him whether he can hear the sound equally well in both ears or better in one ear.
Further investigations
If a specific condition is suspected to be causing the dizziness, further tests may help with the diagnosis. Some examples:
- Schellong test (for circulatory testing) or tilting table examination (for testing the position-related blood pressure adjustment using a movable couch)
- Long-term blood pressure measurement
- X-rays of the cervical spine
- Computed tomography (CT)
- Magnetic resonance imaging (MRI)
- Electroencephalography (EEG): Measurement of electrical brain activity
- Ultrasound examination (Doppler sonography) of the arteries
- Measurement of CSF pressure (pressure of the cerebral fluid) during lumbar puncture
- Evoked potentials (EP): targeted triggering of bioelectrical brain activities as a reaction to certain stimuli, e.g. motor evoked potentials (MEP) and sensory evoked potentials (SEP)
- Blood tests
- Cardiac ultrasound
- Electromyography (EMG), an examination of the conduction of stimuli into the muscles
- Electronurography (ENG), a test used to test the function of peripheral nerves
- Carotid pressure test to examine the blood pressure reflex of the carotid artery
Dizziness: Therapy
Treatment for dizziness depends on its cause. In some cases, for example, certain medications can help reduce dizziness. For other sufferers, physiotherapy, psychotherapy or, in exceptional cases, an operation are possible. Sometimes, however, small aids are sufficient. If the dizziness is based on unstable blood pressure, compression stockings can prevent some attacks.
Therapy for positional vertigo
The doctor can slowly turn the patient's head into certain positions so that the small stones or crystals leave the semicircular canals of the equilibrium organ. These positioning maneuvers are named after their discoverers Epley, Semont and Gufoni. If the person affected also trains their sense of balance in physiotherapy, this can accelerate healing.
Therapy for vestibular neuritis
Glucocorticoids ("cortisone") such as methylprednisolone improve the sense of balance. In addition, targeted balance exercises can reduce dizziness.
Therapy for Menière's disease
In Menière's disease, dizziness can be prevented with medication, for example with high-dose betahistine treatment. This active ingredient lowers the overpressure in the cochlea and can thus reduce dizziness. Alternatively, the doctor sometimes injects the strong antibiotic gentamicin into the inner ear.
Therapy for vestibular paroxysmia
Here, too, you can prevent dizziness with medication. The active ingredients carbamazepine and oxcarbamazepine are suitable for this. Both reduce the over-excitability of the nerves and are also used against epilepsy.
Therapy for motion sickness
So-called antivertiginous drugs (e.g. drugs with the active ingredient dimenhydrinate) can suppress dizziness and nausea. However, they are not suitable for every dizziness and also not for long-term treatment.
Antivertiginous drugs fall into the group of antihistamines (allergy drugs), antidopaminergics or anticholinergics.
Therapy for dizziness in old age
How the doctor treats dizziness in old age depends on the trigger. If he discovers an underlying disease, he will treat it. For example, heart disease, high or low blood pressure can often be treated with appropriate medication.
The active drug dimenhydrinate successfully alleviates acute symptoms of dizziness. Medicines containing ginkgo as well as the active ingredient betahistine, which is supposed to lower the overpressure in the cochlea, can stimulate the blood circulation and metabolic activity of the equilibrium organ in the inner ear in the long term and thus reduce dizziness.
Physiotherapy can help with benign positional dizziness: The special exercises described above also help against dizziness in old age.
In order to avoid falls with (serious) injuries, elderly vertigo patients should use aids such as walking sticks or walking frames / walkers.
Therapy for phobic vertigo
Antidepressants in combination with behavior therapy can help combat mental attacks of dizziness.
Dizziness: You can do that yourself
There are several things you can do yourself to prevent dizziness. You should regularly train your sense of balance, for example by standing on one leg while brushing your teeth or walking on an imaginary line. Numerous sports (such as Pilates, yoga, inline skating, skiing) also strengthen the sense of balance. In addition, the training protects against many causes of dizziness.
In addition, you should pay attention to the following:
- Avoid excessive physical exhaustion.
- Drink enough to stabilize blood pressure.
- Eat regularly to avoid hypoglycaemia.
- Get enough sleep.
- Reduce stress, for example through relaxation exercises.
- Refrain from excessive alcohol and nicotine consumption.
- Check your blood pressure.
- Do not get up too quickly from a sitting or lying position.
- Check the package leaflets for the medications you are taking for dizziness as a possible side effect.
- Diabetes patients should check their blood sugar levels regularly.
Positional vertigo exercises
If you suffer from positional dizziness, you can perform the Epley and Semont maneuvers or the Brandt and Daroff positional vertigo exercises to reduce the attacks of dizziness. Let your doctor show you the exercises beforehand and perform them a few times under his guidance.
Tips against motion sickness
To prevent nausea and dizziness when traveling by boat, in the bus or in the car, simple behavioral tips are sometimes sufficient: if possible, look straight ahead (in the direction of travel) and fix the horizon in the direction of travel if there are fluctuations. Then the organ of equilibrium can synchronize with the eye and you will not get dizzy as quickly.
You may also be able to take motion sickness medication to prevent dizziness and nausea while out and about.
Prevention of dizziness in old age
There are no home remedies such as potato wraps or the like for dizziness in old age.
But you can actively do something to prevent the vertigo from occurring in the first place. This includes: keep moving. Because those who remain physically and mentally active in old age, for example, improve the blood circulation in the inner ear, thereby keeping the equilibrium organs there efficient and can reduce the symptoms of dizziness in old age. In addition, exercise strengthens muscles, joints and bones and improves body awareness, all of which are often impaired by dizziness in old age or dizziness in old age.
But you don't have to become a top athlete to prevent dizziness in old age. Exercises that you can easily do at home - some even while sitting - can help counterbalance disorders in old age. Some examples:
- Look alternately up and down without moving your head.
- Follow a pencil with your gaze and move it back and forth in front of your face.
- While sitting in a chair, bend forward to pick up an object from the floor.
- Tilt your head towards your chest, neck, right and left shoulders, one at a time.
These simple exercises can help prevent or relieve dizziness in old age.
Additional information
Books:
- Vertigo without finding: Systematic training for balance and security by Thomas Weiss, Südwest Verlag
Guidelines:
- Guideline "Acute Dizziness in Family Practices" of the German Society for General Medicine and Family Medicine













.jpg)