Breast augmentation
Martina Feichter studied biology with an elective subject pharmacy in Innsbruck and also immersed herself in the world of medicinal plants. From there it was not far to other medical topics that still captivate her to this day. She trained as a journalist at the Axel Springer Academy in Hamburg and has been working for since 2007 - first as an editor and since 2012 as a freelance writer.
More about the experts All content is checked by medical journalists.
Breast augmentation (breast reconstruction) after an amputation restores the shape of the breast and the nipple. Breast augmentation can also be useful after a breast-conserving operation in which a lot of tissue was removed. The reconstruction takes place with implants or own tissue. Read more about breast augmentation here!
ICD codes for this disease: ICD codes are internationally recognized codes for medical diagnoses. They can be found, for example, in doctor's letters or on certificates of incapacity for work. D05C50
General information on breast augmentation
After a mastectomy (mastectomy), many women want to conceal the procedure - i.e. the absence of one or both breasts. In addition to breast prostheses, there is also a permanent solution: breast augmentation (breast reconstruction). During this plastic-reconstructive operation, the shape of the breast and the nipple are restored - either with implants or with the patient's own tissue. If a breast that has been amputated on one side is reconstructed, the remaining breast often has to undergo a matching operation - so that the end result is symmetrical.
According to the current state of knowledge, the breast augmentation does not seem to have any effects on the course of the disease or the recognition of relapses (local recurrences). However, this cannot be said with certainty because there are no relevant studies.
Breast augmentation: the right time
In principle, breast augmentation can be performed at any time - either in combination with the mastectomy (primary reconstruction, one-stage procedure) or as a separate procedure at a later point in time (secondary reconstruction, two-stage procedure). A primary reconstruction (immediately after the amputation) is less psychologically stressful for some women.
Other patients, on the other hand, want to recover from the mastectomy first and take a leisurely look at the various plastic surgery options before undergoing breast augmentation. Further therapy planning also has an influence on the optimal time for breast augmentation, e.g. whether radiation therapy is planned after the amputation.
Breast augmentation: which procedure?
There are different methods for breast augmentation: on the one hand, reconstruction with implants (mostly silicone implants) and, on the other hand, various procedures for breast augmentation with autologous tissue. You can also combine both. Which procedure is most suitable in each individual case depends not only on the needs and wishes of the woman but also on medical criteria.
These include, for example, the general state of health, the size of the breast, tissue and scar conditions on the operated breast as well as further therapy planning. Radiation therapy, for example, puts a lot of strain on the skin in the breast area, which must be taken into account when choosing a procedure for breast reconstruction.
Breast augmentation with implants
For breast augmentation with implants, doctors usually use plastic pillows with a silicone gel filling. They are considered safe, even if there have been reports in recent years about problems with cheap implants and about implants with unapproved fillers. It is also unclear whether silicone implants cause diseases such as cancer - in any case, such diseases would be very rare.
There are also implants that are filled with a saline solution. Such implants are usually only used as a temporary solution. Other implants are hardly or not at all used in Europe today (e.g. water-based hydrogel implants, breast implants with soybean oil).
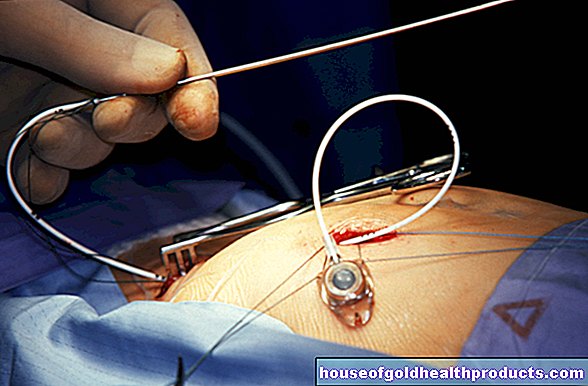
This is how the breast implant is inserted
The implants are pushed under the skin, either over or under the pectoral muscle. In some women, the skin is too tight after the surgical wound has healed. Then it must be stretched with an expander before the implant is inserted: This refillable plastic bag is inserted empty under the skin and then gradually filled with saline solution (via a valve with an injection needle). The skin is stretched so slowly. After a few months, the expander can be removed and the actual implant inserted.
Durability of silicone implants
Modern breast implants are considered safe and durable. However, some of them do not last a lifetime. Especially if the implant is used in younger women, it may need to be replaced after a few years. In any case, it is advisable to have the breast implant checked regularly by a doctor. If there is pain, breast reduction, lumps, or bumps in the breast, women should see a doctor. There may be a faulty implant behind it.
Breast augmentation with implants: advantages and disadvantages
Breast augmentation with implants is a relatively short, simple operation that involves few risks. Compared to breast reconstruction with autologous tissue, it usually causes less pain and there are no additional large scars (e.g. on the abdomen or back due to the removal of autologous tissue). The wound healing is completed quite quickly.
Some women take some time to get used to the breast implant. There are also women who report a feeling of coldness in the chest after inserting the implant.
In response to the silicone implants, the body surrounds them with connective tissue. This can lead to hardening, which in the worst case compresses the implant, causing pain and deformation of the breast. In the case of such capsular contracture, the implant is usually replaced.
Radiation therapy can be problematic with breast implants.
Breast structure with own tissue
Breast reconstruction is also possible with your own tissue: To do this, the doctor takes a skin and fat flap with or without muscles from another part of the body and forms the new breast from it.
Operations with muscles
A TRAM flap (transverser rectus abdominalis flap) is often used to build up the breast with the patient's own tissue: a flap of skin and adipose tissue is removed transversely from the lower abdomen together with part of the straight abdominal muscle. It can be transplanted into the chest area as a "pedunculated" or "free" flap:
With a “pedicled” TRAM flap, the supplying vessels are not severed. They have to be long enough so that the skin-adipose tissue-muscle flap can be pivoted up to the chest.
With a "free" flap, the vessels are severed. After it has been transplanted into the chest area, the flap must be sutured with new blood vessels using microsurgery so that the tissue is adequately supplied.
Alternatively, a skin-adipose tissue-muscle flap from the area of the large back muscle (LADO = musculus latissimus dorsi) or - in exceptional cases - from the thigh (TMG = transverse musculocutanaeus gracilis) is used to augment the chest.
Operations without muscles
The DIEP flap (DIEP = deep inferior epigastric perforator) consists of deep skin and fat tissue from the abdomen, but without muscles. Sometimes a superficial flap of skin and adipose tissue is removed from the abdomen (SIEP = superficial inferior epigastric artery).
Women who are very slim often do not have enough fat on their abdomen. Skin and fatty tissue from the lower or upper bottom can then be used to build up the breast (I-GAP = inferior gluteal artery perforator; S-GAP = superior gluteal artery perforator).
Breast augmentation with own tissue: advantages and disadvantages
Breast reconstruction with autologous tissue usually looks natural and is more permanent than the insertion of breast implants. Subsequent corrections are very rarely necessary. In addition, with this type of breast augmentation there are no problems with radiation therapy.
On the other hand, building up the breast with your own tissue is more complex and associated with more complications than the insertion of implants. Sometimes reoperations are necessary. In addition, the tissue removal leaves larger scars on the affected part of the body.
The removal of a tissue flap with muscles (as with the TRAM flap) has the disadvantage that movement restrictions, muscle weakness and pain can occur in the removal area. This is not the case when removing a tissue flap without muscles (as with the DIEP flap).
The latter procedure is more complex and requires special experience from the surgeon: He has to create a new vascular supply for the tissue flap. In addition, with breast reconstruction with a tissue flap without muscles, the risk of tissue death (necrosis) is greater than with the use of a tissue flap with muscles or implants.
Experimental: breast augmentation with autologous fat
Today there is also the method of reconstructing an amputated breast using only one's own fat (without skin and muscles). The surgeon obtains the fat for the breast augmentation by suctioning it from the abdomen, back or hips. It has to be injected into the chest several times because it is partially broken down by the body.
Reconstruction of the nipple
As soon as the breast has completely healed after the reconstruction (which usually takes several months), the nipple can still be reconstructed. The waiting time is necessary because the reconstructed breast often changes slightly after the procedure. For example, the skin can give way slightly when implants are inserted, and a breast reshaped with its own tissue can sag a little.
The nipple can be reconstructed either with your own skin tissue (e.g. from the other nipple or the abdomen) or by means of a tattoo (in a specialized clinic or practice).
The cost of breast augmentation
As a rule, the costs for common breast augmentation procedures after breast cancer are covered by statutory health insurance companies. Privately insured persons should discuss the assumption of costs with their health insurance company in advance.
Tags: organ systems gpp healthy workplace