Achalasia
Dr. med. Julia Schwarz is a freelance writer in the medical department.
More about the experts All content is checked by medical journalists.Achalasia is a rare chronic disease of the esophagus. Those affected mainly suffer from discomfort when swallowing. Other typical achalasia symptoms are belching of undigested food from the esophagus, pain behind the breastbone, weight loss and bad breath. If left untreated, achalasia can cause serious complications. Read everything you need to know about the signs, risks, and treatment options for achalasia here.
ICD codes for this disease: ICD codes are internationally recognized codes for medical diagnoses. They can be found, for example, in doctor's letters or on certificates of incapacity for work. Q39K22
Achalasia: description
Achalasia is a disease of the gullet (esophagus) that makes it difficult for people to swallow. When swallowing, the contraction movements of the esophagus are normally exactly synchronized with the time at which the lower sphincter opens: "La Ola waves" -like movements of the esophagus carry the food pulp through the esophagus. At the lower end, the sphincter relaxes at exactly the right time and the food can get into the stomach. In achalasia, on the one hand, the contraction movements (peristalsis) of the esophagus are generally weakened and, moreover, no longer precisely coordinated with the lower sphincter muscle. On the other hand, the sphincter muscle is permanently tense (Greek achalasis = lack of relaxation), so it can no longer expand sufficiently.
As a consequence, the food pulp is no longer transported normally through the esophagus due to the disturbed peristalsis. In addition, it accumulates in front of the permanently tense lower esophageal sphincter, which causes the typical achalasia symptoms. These include, in particular, difficulty swallowing solid food (dysphagia) and choking up undigested food particles from the esophagus into the oropharynx.
Achalasia: who is affected?
Achalasia is rare. Every year about one in 100,000 people gets achalasia. Most people in middle age, i.e. between the ages of 30 and 50, are affected. Sometimes, however, children, adolescents or the elderly also get sick. If achalasia occurs in childhood, a genetic cause such as the so-called triple A syndrome is often responsible.
Differentiation between primary and secondary achalasia
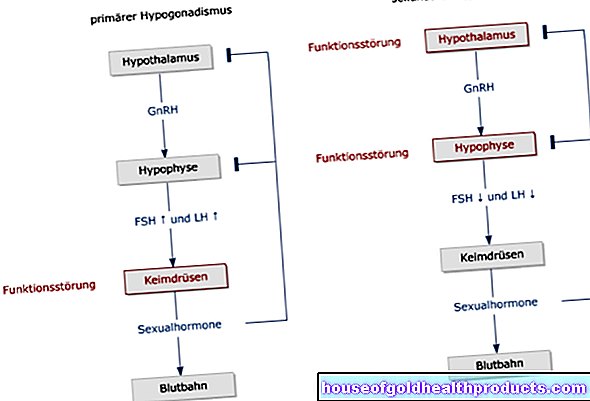
Doctors differentiate between primary and secondary achalasia. Primary achalasia is the most common type. Doctors call it primary achalasia when the cause of the achalasia cannot be clearly identified. How primary achalasia develops is still unclear. In the rarer secondary achalasia, however, there are clear causes such as esophageal cancer or Chagas disease. These diseases damage the nerve tracts in the area of the esophagus, so that the normal function of the esophageal contractions and the esophageal sphincter is disturbed. It is typical of secondary achalasia that swallowing difficulties increase much faster than in primary achalasia. Older people are more likely to be affected by secondary achalasia.
Achalasia: symptoms
The typical signs of achalasia are difficulty swallowing (dysphagia) and belching of undigested food (regurgitation). There are also other complaints such as pain behind the breastbone, weight loss and bad breath.
Achalasia Symptoms - Difficulty Swallowing
Initially, the symptoms are usually mild and occur only sporadically. In the early stages of the disease, patients only experience problems swallowing solid food. While swallowing, they have the feeling that the food is stuck in their throats and drink accordingly. Increasing the amount of water you drink means that the food can get better into the stomach. In addition, some sufferers feel a feeling of pressure in the chest region behind the sternum. In an advanced stage of the disease, liquids can no longer be swallowed or only with difficulty. This poses considerable problems for those affected. On the one hand, the swallowing disorder is emotionally very stressful, on the other hand, those affected lose a lot of weight, which significantly reduces their physical performance.
Achalasia Symptoms - Belching of undigested food particles
In the advanced stage, achalasia leads to unwanted belching. Often undigested food remains from the esophagus back into the mouth. The spontaneous burping of undigested food residues occurs particularly frequently when the patient is lying down and the effect of gravity no longer acts as a “brake”.
Some patients feel very bloated and also vomit. The patients lack the bitter taste in the mouth that is typical of reflux disease, since the food in achalasia has not yet come into contact with the gastric acid. Since the lower esophageal sphincter is permanently tense in achalasia, those affected have no or only very rarely heartburn.
Many patients choke on the undigested food when it gets into the windpipe (aspiration). This happens especially at night when the patients are lying down. The reflux of food can lead to coughing attacks at night. In addition, the food particles in the windpipe and bronchi (aspiration) can cause pneumonia.
More achalasia symptoms
With pronounced achalasia, those affected lose a lot of weight. In primary achalasia, body weight decreases slowly over months or years and is usually a maximum of ten percent of the original body weight. In secondary achalasia, the weight loss can be more pronounced and also progress in a much shorter period of time.
Because of their achalasia, some patients also have severe pain behind the breastbone (retrosternal pain), which occurs particularly when swallowing. If very pronounced pain is in the foreground in achalasia, doctors sometimes also refer to this as "hypermotile achalasia".
Because the food pulp builds up in front of the permanently tense lower esophageal sphincter, food remains in the esophagus. These are colonized and broken down by bacteria. As a result, those affected can suffer from pronounced bad breath (foetor ex ore, halitosis).
Achalasia: causes and risk factors
The act of swallowing is a complicated, finely tuned process that requires precisely timed control of the muscles of the esophagus by nerve impulses. If this control fails, the peristalsis of the esophagus is disturbed and the lower esophageal sphincter no longer relaxes.
The causes of primary achalasia are not yet fully understood. There is evidence that achalasia is caused by the destruction of certain nerve tracts and nerve centers (ganglion cells) in the esophagus. The so-called myenteric plexus (Auerbach plexus) appears to be particularly affected. This is a fine network of nerves in the muscle wall of the esophagus, stomach and intestines.
How it comes to the destruction of the nerve cells in primary achalasia is not yet known. For example, researchers consider an infection or autoimmune disease to be possible causes. In the case of secondary achalasia, on the other hand, science has a more concrete idea why nerve cells die: Typical causes of secondary achalasia are esophageal cancer (especially cardiac cancer) and Chagas disease. In both diseases, the nerve cells in the wall of the esophagus are damaged. Chagas disease is a bedbug-borne parasitic disease that occurs mainly in Central and South America and is only likely to play a role in the development of achalasia in Germany in the rarest of cases.
Achalasia is also inherited in rare cases
If children and adolescents are already affected by achalasia, a genetic cause is often responsible. For example, achalasia is one of the main symptoms of what is known as triple A syndrome (AAA syndrome). The disease is inherited as an autosomal recessive trait and, in addition to achalasia, includes other symptoms such as adrenal insufficiency and the inability to produce tears (alacrima). Achalasia is also often observed in Down syndrome (trisomy 21). About two percent of people with Down syndrome suffer from it. In addition, rare genetic diseases such as familial visceral neuropathy and achalasia-microcephaly syndrome are associated with achalasia.
Achalasia: examinations and diagnosis
The right person to contact if you suspect achalasia is your family doctor or a specialist in internal medicine and gastroenterology. With a detailed description of your complaints, you provide the doctor with valuable information about your current state of health (anamnesis). The attending physician could ask you the following questions:
- Do you have difficulty swallowing, such as feeling like food is stuck in your throat?
- Does this feeling improve when you drink fluids?
- Do you occasionally have to dig up undigested food residues?
- Does it hurt when you swallow?
- Have you lost weight?
- Have you noticed bad breath?
The doctor will then examine your stomach and upper body in particular and shine a light into the mouth and throat in order to detect any changes. He will also feel your throat. He can, for example, determine enlarged lymph nodes on the neck (indicating an inflammation or a tumor) and feel the thyroid gland. In order to be able to diagnose achalasia with certainty, further examinations are usually necessary.
Supplementary examinations if achalasia is suspected
Achalasia can often be diagnosed by the typical symptoms in combination with imaging tests such as the esophagus and the so-called porridge swallow. If necessary, the function of the lower esophageal sphincter can also be checked with the esophageal manometry.
Esophagus and gastroscopy (esophagoscopy and gastroscopy)
The structure of the mucous membranes in the esophagus and stomach can be assessed with the help of a reflection through an endoscope. In addition, the reflection serves to rule out other diseases of the esophagus and stomach such as inflammation, scarring or cancer. The patient is not allowed to eat or drink anything for six hours before the examination so that the doctor has a clear view of the mucous membranes during the examination. Normally the esophagus is then completely free, but in achalasia there are often leftovers in the esophagus. If achalasia is suspected, a tissue sample should always be taken during the endoscopic examination to rule out a malignant tumor.
Esophageal swallow examination
The so-called esophageal swallow is a method for displaying the act of swallowing with the help of an X-ray machine and a contrast medium. The patient swallows a porridge enriched with a contrast agent (usually barium sulfate). While swallowing, the patient's throat and chest are X-rayed. If achalasia is present, the x-ray often shows a champagne glass-shaped transition between the esophagus and the stomach entrance. The entrance to the stomach is thinned in the shape of a pedicel, while the esophagus in front of it is widened in the shape of a funnel. This champagne glass shape arises because the food pulp builds up in front of the constriction of the lower esophageal sphincter and thus the esophagus in front of the constriction is expanded over time.
Pressure measurement of the esophagus (esophageal manometry)
With the help of a pressure measurement of the esophagus (manometry), the peristaltic movements of the esophagus and the function of the esophageal sphincter can be determined. For this purpose, a probe with several measuring channels of the gastric outlet is advanced and the pressure is determined at various points in the esophagus during the swallowing process. In achalasia, the normal contraction movements of the esophagus are uncoordinated and weakened and the lower esophageal sphincter constantly exerts excessive pressure on the probe because it does not relax.
Achalasia: treatment
Achalasia treatment is necessary if the disorder causes discomfort. There are several options available to alleviate the achalasia symptoms. With the help of medication or special interventions, an improvement in the symptoms can usually be achieved. The aim of therapy is to reduce the increased pressure in the lower esophageal sphincter. A complete cure is hardly possible, however, as once damaged nerve cells only regenerate to a limited extent.
Achalasia Drugs
Drug therapy only helps about ten percent of patients. The active ingredient nifedipine - originally a drug used to treat high blood pressure - relaxes the esophageal sphincter muscle. The active ingredient group of nitrates has a similar effect. The medication is taken about 30 minutes before food is consumed. Thus, the lower esophageal sphincter relaxes in time and the food can get into the stomach more easily. However, with prolonged treatment, the drugs become less effective and further procedures become necessary.
Achalasia - special interventions
The narrowed transition between the esophagus and the stomach can be widened using various methods. Of these, balloon dilatation is the method of first choice. Young patients with achalasia are an exception, for whom an operation is usually more sensible.
An injection of botulinum toxin directly into the lower esophageal sphincter is also often done. Surgical stretching of the junction between esophagus and stomach is only carried out in a few cases.
Balloon expansion (balloon dilatation)
The narrowing of the junction between the esophagus and stomach can be stretched with the help of a balloon. The balloon dilatation can be performed during a gastroscopy, so no surgery is necessary. The doctor pushes a thin tube over the mouth into the esophagus up to the constriction (stenosis) at the entrance to the stomach. There the small balloon at the end of the tube is inflated. This stretches the stenosis, which leads to an improvement in symptoms in 60 percent of those affected. In rare cases (around five percent), complications during the procedure can tear the esophagus or the stomach entrance. If bacteria penetrate the wound, it can cause esophagitis. In addition, balloon dilatation has to be repeated after a few years in about half of the cases.
Botox injection
The injection of diluted botulinum toxin (Botox) into the narrowed esophageal sphincter can also be performed during a gastroscopy. Most people know Botox as a nerve crippling poison from cosmetic medicine. In the esophageal sphincter it blocks the nerve tracts, causing the sphincter to relax. This type of achalasia therapy improves symptoms in 90 percent of those affected. However, achalasia symptoms recur in many patients after just a few months. There are not yet enough long-term studies to be able to reliably assess the value of this form of treatment for achalasia.
Surgery (myotomy)
If the patient cannot be helped adequately with the above measures, surgery could also be used. This is particularly useful for young patients, as balloon dilatation is often poor in this age group.
In a myotomy, the lower, ring-shaped esophageal sphincter is severed. Since the mucous membrane must not be injured, this muscle transection can only be carried out through an access route from outside the esophagus. Most often, the surgeon chooses access via an incision in the chest (transthoracic) or upper abdomen (transabdominal). Myotomy is a very effective method. In addition to severing the esophageal sphincter, anti-reflux surgery is also performed in the same operation. Its purpose is to prevent acidic gastric juice from flowing back into the esophagus.
Achalasia: disease course and prognosis
Achalasia is a chronic disease that unfortunately does not heal spontaneously. The swallowing difficulties typical of achalasia usually increase over years or even decades. With the help of various treatment options, however, the symptoms can usually be sufficiently alleviated.
Achalasia Complications
If left untreated, achalasia can lead to a steadily widening (dilatation) of the esophagus. In extreme cases, a so-called megaesophagus forms, which is no longer able to transport the chyme from the mouth to the stomach. The increased belching can trigger inflammation of the esophagus (esophagitis) or complications of the lungs (dry cough, hoarseness and even pneumonia).
Achalasia is associated with an increased risk of cancer of the esophagus (esophageal cancer). The risk of achalasia patients developing a malignant tumor of the esophagus is 30 times higher than that of healthy people. This is due to the fact that with constant stress and irritation of the esophageal mucosa, new cells must constantly form to repair the esophageal mucosa. The increased rate of cell division means an increased risk of cell degeneration. Achalasia patients should therefore be examined regularly even after successful treatment.
Tags: healthy feet gpp organ systems
.jpg)