bulimia
and Christiane Fux, medical editorJulia Dobmeier is currently completing her master's degree in clinical psychology. Since the beginning of her studies, she has been particularly interested in the treatment and research of mental illnesses. In doing so, they are particularly motivated by the idea of enabling those affected to enjoy a higher quality of life by conveying knowledge in a way that is easy to understand.
More about the expertsChristiane Fux studied journalism and psychology in Hamburg. The experienced medical editor has been writing magazine articles, news and factual texts on all conceivable health topics since 2001. In addition to her work for, Christiane Fux is also active in prose. Her first crime novel was published in 2012, and she also writes, designs and publishes her own crime plays.
More posts by Christiane Fux All content is checked by medical journalists.
Bulimia is a mental illness that is an eating disorder. Those affected have recurring food cravings in which they eat uncontrollably. After such "binge eating" they are very afraid to gain weight. As a result, they vomit, take laxatives, or exercise excessively. Read here what bulimia is, how to recognize it and how to treat it.
ICD codes for this disease: ICD codes are internationally recognized codes for medical diagnoses. They can be found, for example, in doctor's letters or on certificates of incapacity for work. F50
Brief overview
- Description: widespread eating disorder with alternation from strictly controlled eating habits and food cravings
- Main symptoms: "Seizures" with subsequent vomiting, excessive sport, fasting
- Possible consequences: malnutrition, tooth damage, gastritis, inflamed esophagus, cardiac arrhythmia, kidney damage, osteoporosis
- Causes: weak self-esteem, striving for recognition, adaptation to the prevailing ideal of beauty, familial influence on eating behavior and self-acceptance, genetic causes, biological triggers
- Diagnostics: standardized questionnaires and interviews on symptoms and causes
- Therapy: cognitive behavioral therapy, relearning healthy eating habits, individual and group therapy, antidepressants, mostly inpatient treatment
Bulimia: description
Bulimia (bulimia nervosa) is one of the eating disorders. Colloquially it is also referred to as eating-vomiting addiction. Typical bulimia symptoms are food cravings, in which those affected devour large amounts of food in an uncontrolled manner. In order not to gain weight, they then take drastic countermeasures.
Psychological backgrounds
People with bulimia strive for a figure that corresponds to the prevailing, overly slim ideal of beauty. This way they hope for recognition and affection. It seems threatening to them to gain weight because they fear exclusion. Often, a diet is the beginning of the vomiting addiction.
Bulimia: symptoms
Bulimia is not as easy to recognize for outsiders as anorexia, for example. People who suffer from eating-vomiting addiction are usually normal or only slightly underweight. Some are even overweight. The eating-vomiting attacks usually take place in secret, so that no one notices anything for a long time.
Most of the time, bulimics have a strong control over their eating habits. You are on a diet and skip meals. But then they keep getting hunger pangs.
-
Bulimia: "Offer Help"
Three questions for
Dr. med. Robert Doerr,
Specialist in psychiatry, psychotherapy -
1
Who Is Particularly Affected by Eating Disorders?
Dr. med. Robert Doerr
Women in particular are significantly more likely to develop eating disorders. Likewise, low self-esteem, excessive performance demands and problematic family behavior patterns contribute to the development. However, the trigger is rarely a single factor; rather, various factors work together, and there is often a one-off triggering event, such as a diet.
-
2
What is the best way to address a suspicion of bulimia?
Dr. med. Robert DoerrPreferably very directly. Say you are worried. Avoid eating criticism and accusations. Speak in the first-person form and do not apply pressure. Instead, signal that the person means a lot to you and that you want to help. Getting help is not a sign of weakness, but the first important step towards change.
-
3
Can people with bulimia get completely well again?
Dr. med. Robert DoerrRelapses can occur especially at the beginning and in the first year after the end of treatment, the probability is around 30 percent. It is helpful to develop an understanding of the risk situations. And to develop concrete, well-functioning coping strategies. Also, don't evaluate a relapse as a complete failure, but as an incident from which you can learn something for the future.
-
Dr. med. Robert Doerr,
Specialist in psychiatry, psychotherapyDr. med. Robert Doerr is chief physician at the Schön Klinik Berchtesgadener Land in the field of psychosomatic medicine.

Repeated episodes of binge eating
Bulimic people lose control during food cravings. They gobble up large amounts of very high calorie foods in a short amount of time. The loss of control can be so severe that they are initially unaware of their actions. Bulimics sometimes consume up to 10,000 calories in about one to two hours. That is more than four times what a healthy person needs in a full day. Women have a requirement of around 1900 kilocalories per day.
The feeding attacks are often triggered by stress and last until an unpleasant feeling of fullness arises. While devouring the food, some sufferers feel a brief relaxation. After the binge eating, however, they are usually ashamed of their behavior, feel disgusted or reproach themselves.
Measures against weight gain
In order not to gain weight, people with bulimia try to get the food out of the body as undigested as possible or to take other countermeasures. There are two types of bulimics:
Countermeasure vomiting (purging type): About 70 to 90 percent of bulimics belong to the "purging type". In most cases you will vomit up what you have eaten immediately. To do this, they provoke nausea with their fingers. Some patients also use aids, such as wooden spoons, the handles of which they stick into their necks. Some instead (or in addition) try to maintain their weight through fasting, laxatives, or extreme exercise.
To check that they have vomited all of their food, many bulimic patients eat a colored food, such as tomatoes, at the beginning of the binge eating.
Some purging-type bulimics also use laxatives or make enemas.
Countermeasure Fasting and Exercise (non-purging type): Patients of the "non-purging type" do not reduce their weight by vomiting, but by fasting and excessive physical activity. However, this type is rarer than the purging type.
Pay attention to your figure and weight
Similar to anorexics, people with bulimia are very careful about their weight and are very afraid of gaining weight. Outward appearance is crucial to their self-esteem. They only find slim bodies beautiful. The exaggerated fixation on figure and nutrition is often the first symptom that strangers to the outside world.
Differences Between Bulimia and Anorexia
Bulimia and anorexia nervosa are not always easy to distinguish. In fact, bulimia often begins with a period of severe weight loss before the binge eating and vomiting. The psychological backgrounds of the illnesses, however, are fundamentally different.
|
bulimia |
anorexia |
|
The aim is to have a very slim figure (slightly underweight) |
A person who is severely underweight and viewed by others as unhealthy and unattractive is perceived as ideal |
|
Longing for recognition and belonging |
Striving for demarcation, self-control |
|
Weight loss in order to meet the prevailing ideal of beauty |
Weight loss and refusal to eat as an expression of self-control, asceticism |
|
Fear of abandonment, exclusion |
Fear of losing control and being overwhelmed |
|
Shame for the illness |
Proud of the ability to perform asceticism |
|
Maintains sexual partnerships |
Only rarely sexual partnerships |
|
Serious secondary diseases are possible, fatal complications are rare |
High risk of fatal progress |
Bulimia: consequences
Pronounced bulimia causes great damage in the body.
Consequences of bulimia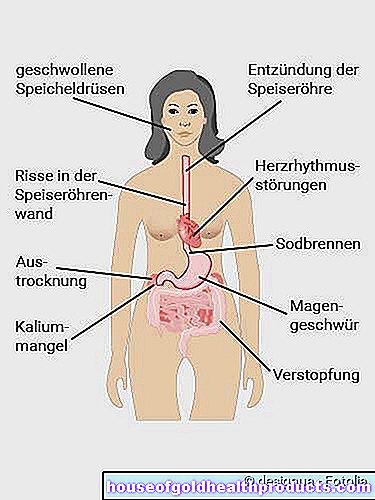
- Malnutrition: Repeated diets, constant vomiting, but also the use of laxatives can disrupt the electrolyte balance and cause malnutrition.
- Heart failure: too low a potassium level in the blood and cells can cause an irregular heartbeat and heart failure.
- Osteoporosis: calcium deficiency makes bones fragile.
- Kidney damage: The lack of electrolytes can cause life-threatening kidney damage.
- Abdominal pain and torn stomach: Overeating causes the stomach to bloat. This causes a lot of pain. In the worst case, a life-threatening tear in the stomach (gastric rupture) can occur.
- Constipation: Vomiting slows down the transport of food in the body. Blockages occur.
- Tooth damage: The consequences of bulimia are often felt in the teeth. The stomach acid first destroys the tooth enamel and then the dentin. As a result, the teeth can initially become painful and temperature-sensitive and then damaged.
- Esophagitis: The rising stomach acid causes inflammation of the lining of the esophagus (esophagitis). In extreme cases, if gastric juice gets into the airways, there is a risk of suffocation or pneumonia.
- Gastritis: In addition, vomiting irritates the stomach and can also become inflamed (gastritis). Constant vomiting then often leads to further injuries up to painful bleeding, scarring and organ ruptures.
- Inflammation of the pancreas: The eating attacks can lead to inflammation of the pancreas. It manifests itself in severe abdominal pain, fever and an increased heart rate.
- Menstrual Disorders and Infertility: Often times, women with bulimia have irregular or no menstrual periods. Fertility also decreases.
- Skin changes: In 10 to 30 percent of bulimic patients, dry skin and brittle hair with hair loss are further consequences. Frequent vomiting causes the salivary glands to swell and the corners of the mouth to become sore.
- Mental changes: bulimia affects mood and concentration. In half of those affected, the shape of the brain also changes (pseudo-atrophy). However, the causes and effects of this phenomenon are not clear.
- Risks in pregnancy: Due to malnutrition, unborn children of a bulimic mother often do not develop properly. The child can suffer permanent damage.
Bulimia: causes and risk factors
Why a person gets bulimia is not yet fully understood. When the disease breaks out, several factors often come together. Risk factors include:
- genetic predisposition
- biological components
- lack of self-esteem
- problematic family influences
- high performance standards
- western ideal of beauty
- negative self-image
People with bulimia often have a negative self-image. There is a deep gap between the claim "how I want to be" and the perception of "how I really am". This is especially true for your own body. Self-esteem depends heavily on the figure. Bulimics usually strive for an extremely slim ideal, which they can only achieve by massive restriction in eating - or by vomiting.
Extreme performance demands
Patients' self-esteem depends heavily on their success in achieving lofty goals.At the same time, they are extremely self-critical, which leads to constant dissatisfaction with their own performance.
The conflict between excessive expectations of oneself and fear and feelings of failure creates strong states of tension. The binge eating can relieve this tension for a short time.
Problematic family behavior
How food is handled within the family can contribute to eating disorders. It is particularly critical when eating serves to distract, reward or relax.
Restrained eating behavior and frequent diets by mothers also seem to have a negative influence, as does a critical attitude towards one's own body within the family.
Often there are problems in dealing with family members. According to some experts, bulimics more often come from families that are particularly ambitious and performance-oriented or who resolve their conflicts impulsively and violently.
Some experts also describe a lack of warmth, affection and appreciation in family dealings with one another.
All of this may or may not be the case. It is also unclear whether such family constellations actually contribute specifically to bulimia or generally promote emotional instability.
Western ideal of beauty
Bulimia is often fueled by a desire to conform to society's ideals of beauty. The current ideal is strongly towards underweight. It also motivates people of normal weight to go on a diet.
Often, patients with bulimia are slightly overweight before the onset of the eating-vomiting addiction. They then feel unattractive and find it difficult to accept their bodies. They try to get closer to the ideal of beauty through diets. Often this is the beginning of bulimia.
Constant starvation greatly fuels the need for food. Eventually they can no longer withstand the pressure and the vicious circle of eating-vomiting addiction begins. The momentum of bulimia can then only be stopped with professional help.
Biological factors
Serotonin: This messenger substance creates feelings of happiness, but it also influences the feeling of satiety in the brain. It has been found that people with bulimia produce less serotonin.
Since the body needs carbohydrate-rich food for the formation of the messenger substance, this is a possible explanation for the binge eating: People with bulimia try to regulate negative feelings through the massive intake of carbohydrates. However, it is unclear whether the disturbance in the messenger system is actually the cause of bulimia or rather occurs in the course of bulimia and stabilizes it.
Endogenous opioids: Endogenous opioids also appear to play a role in bulimia. These are substances that reduce or suppress the sensation of pain and appetite.
It is believed that high opioid levels make fasting easier when you are hungry and at the same time lift your mood. Researchers have found very low levels of endogenous opioids in bulimics. This triggers cravings and thus also the binge eating. In this way, low opioid levels could contribute to bulimia.
Genetic causes
There is also a hereditary predisposition to the eating disorder. This is particularly indicated by twin studies. If one twin falls ill, the other has a much higher risk of developing bulimia in identical twin pairs than in dizygotic twins.
How great the influence of the genes actually is, however, is not yet certain. Overall, however, it does not seem as great in bulimia as it does in anorexia (anorexia).
Bulimia: examinations and diagnosis
If bulimia is suspected, it makes sense to see your family doctor first. He can refer you to specialized doctors and psychologists.
The doctor can find out whether a patient suffers from bulimia during an anamnesis interview. The doctor could ask the patient the following questions if bulimia is suspected:
- Do you feel too fat?
- Are you happy with your body?
- Do you pay close attention to how much and what you eat?
- Do you have food cravings that make you feel like you can't stop eating?
- Does it happen that you vomit the food you have eaten again? How common is that?
- Do you have physical complaints such as muscle weakness, constipation, severe bulging pain?
Most of those affected hide their eating and vomiting behavior. Many are not sure whether this is pathological at all. Others mistakenly believe that they can get a grip on the pathological behavior themselves. It is a great challenge for the patient and the doctor alike to build such trust that the person concerned can open up to the doctor and seek help.
Psychological diagnostics
If the family doctor determines bulimia, he will provide the person concerned with psychotherapeutic help. Since bulimia has predominantly psychological causes, treating the physical complaints is not sufficient.
The psychotherapist can use a clinical interview to record the specific psychological complaints. He can also determine whether the patient suffers from other disorders. People with bulimia often also have depression, anxiety disorders, or personality disorders.
Diagnostic criteria of bulimia
According to the Diagnostic and Statistical Manual of Mental Disorders (DSM-V), the following characteristics are considered to be signs of bulimia.
- repeated episodes of binge eating
- repeated use of inappropriate countermeasures to counteract weight gain
- The feeding attacks and inappropriate compensatory behavior occur on average at least twice a week for at least three months.
- Figure and body weight have an undue influence on self-assessment.
- Symptoms are not solely associated with anorexia.
To record the diagnostic criteria, special questionnaires have been developed, which are supplemented by interviews. This includes the extensive structured clinical interview for DSM-IV (SKIB interview). In addition to the eating disorder, it also includes other mental illnesses.
The structured interview for anorexia and bulimia (SIAB) consists of a questionnaire for self-assessment as well as an interview part with 87 questions, which the doctor or psychologist goes through with the patient.
Physical examination
In addition to the psychological diagnosis, a physical examination is also necessary.
The doctor also examines the blood, which is often poor in vital salts due to vomiting. He also checks whether the stomach, esophagus and teeth are injured or attacked by stomach acid.
If the lack of salts already shows kidney damage or cardiac arrhythmias, the doctor tests the function of these organs using an EKG, heart echo and an ultrasound of the kidneys.
Bulimia test
There are a number of online offers for the bulimia test on the Internet. Such tests are based on the questions a doctor would ask, for example
- on eating habits and diets
- about the attitude towards one's own body
- to self-esteem
- especially about the feeding attacks themselves
- to self-induced vomiting, laxative consumption and excessive exercise
Only an expert can make a reliable diagnosis for bulimia, but the online tests provide guidance. For example, a bulimia test on the Internet can encourage those affected to think about their eating habits and, if necessary, to seek help.
Bulimia: treatment
Bulimia is a serious mental disorder. However, people with bulimia usually find it difficult to realistically assess their eating behavior, or they do not want to admit that it is disturbed. Therefore, professional help with bulimia is essential. The main goals in the treatment of bulimia are
- achieve a rapid change in eating habits in the short term in order to restore or maintain physical health.
- To help those affected in the long term to recognize the causes of the disrupted eating behavior and to eliminate them or to find other ways to deal with it.
Normalization of eating behavior
In milder cases, bulimia can also be treated on an outpatient basis. In severe cases, however, diet needs to be controlled so that patients can return to healthy eating habits. This is usually only possible in a stationary setting.
Not too much and without vomiting
At the beginning of the treatment, a balanced meal plan is drawn up together with the patient, which he then has to adhere to. This includes eating regular meals - at least three a day. It's about eating without having binge eating or vomiting the food.
Afraid of taking calories
Patients also learn to eat higher calorie foods that they have avoided outside of eating-vomiting attacks without fear. You will also be involved in the preparation of the meal. Handling food should be a positive, relaxed experience for them.
Normalized urge to eat
The physical deficiency is ended by a regular and varied diet. Since the patient no longer goes through phases of hunger, the urge to ingest large amounts of food is also reduced.
psychotherapy
Often, cognitive behavioral therapy is used to treat bulimia.
Realistic body image: Patients should develop a more realistic attitude towards their body and weight. It is also about questioning the social ideals of beauty and slimness.
Looking for a trigger: In collaboration with the therapist, bulimia patients find out which situations lead to an eating-vomiting attack. A food diary can help with this. The therapist then tries, together with the patient, to find alternative ways and behaviors to deal with stressful situations.
Confrontation therapy: In bulimia therapy, so-called confrontations are often used, which serve to reduce fears. The therapist encourages patients to expose themselves to situations or to eat foods that cause them anxiety and which otherwise have triggered a binge eating. The therapeutically supported confrontation leads to a steady reduction in fears and increases the self-confidence and self-esteem of bulimics.
Broad spectrum of therapies
In the case of an inpatient stay, a wide range of therapies for holistic treatment is usually used. This includes:
- Individual therapy
- Group therapy
- Gestalt therapy
- Art therapy
- Exercise therapy
- Music therapy
- Relaxation courses
- Nutritional advice
Medication
At the beginning of bulimia therapy and during crises, some patients are temporarily given antidepressant substances. The drug fluoxetine is mainly used for this purpose. Not only does it have an antidepressant effect, but it also reduces vomiting attacks. Medicines are not suitable as the sole therapy for bulimia.
Bulimia: disease course and prognosis
Bulimia usually begins in adolescence or early adulthood. It is mainly women between the ages of 18 and 30 that get the disease, but young men are also increasingly affected. Bulimia can be preceded by a period of severe weight loss which then turns into vomiting attacks. Often, diets are the starting point for the vomiting addiction.
In the course of the disease, there are always times when people with bulimia eat normally. The number of vomiting and eating attacks varies from person to person. In stressful phases in which the patient is particularly stressed, vomiting attacks occur more frequently.
Often, bulimia is not treated until the patient's third decade - i.e. after a long period of illness. After all, about half of the patients who suffered from bulimia get well, although usually only after several years of the disease.
Additional information
Books:
- Back to life: In 12 steps out of bulimia (Nina Wolf, Tectum Wissenschaftsverlag, 2018)
- The woman who ate in the moonlight: Overcoming eating disorders through the wisdom of ancient fairy tales and myths (Anita Johnston, Knaur MensSana TB, 2007)
Guidelines:
S3 guideline "Eating disorders, diagnostics and therapy" of the German Society for Psychosomatic Medicine and Psychotherapy (DGPM)
Self-help groups:
Cinderella - Counseling Center for Eating Disorders of the Action Group for Eating and Anorexia e.V.
https://www.cinderella-beratung.de/
Tags: prevention symptoms hair