Kallmann syndrome
Astrid Leitner studied veterinary medicine in Vienna. After ten years in veterinary practice and the birth of her daughter, she switched - more by chance - to medical journalism. It quickly became clear that her interest in medical topics and her love of writing were the perfect combination for her. Astrid Leitner lives with daughter, dog and cat in Vienna and Upper Austria.
More about the experts All content is checked by medical journalists.Kallmann syndrome is a congenital disease in which little or no sex hormones are produced. Those affected do not go through puberty; if left untreated, both men and women are sterile. In addition, the sense of smell is usually disturbed: KS patients only smell very limited or nothing at all. Read everything you need to know about the "olfactory syndrome" here!
ICD codes for this disease: ICD codes are internationally recognized codes for medical diagnoses. They can be found, for example, in doctor's letters or on certificates of incapacity for work. E23

Brief overview
- What is Kallmann Syndrome? Congenital developmental disorder that leads to a lack of sex hormones and thus to the absence of puberty. In addition, most patients lack the sense of smell.
- Causes: Congenital genetic changes (mutations)
- Risk factors: The disease occurs in families in around 30 percent of patients.
- Symptoms: Lack of puberty development (underdevelopment of the penis, testicles and prostate, little pubic, armpit and body hair, lack of beard growth, absence of the first menstrual period), infertility, lack of pleasure, sense of smell is absent or greatly reduced, long-term consequence: osteoporosis
- Diagnostics: physical symptoms such as lack of development of secondary sexual characteristics, hormone analysis, genetic testing, ultrasound, magnetic resonance tomography, computer tomography, x-ray
- Treatment: replacement therapy with hormonal drugs
- Prevention: No prevention possible
What is Kallmann Syndrome?
The Kallmann syndrome (KS, olfactogenital syndrome, De-Morsier-Kallmann syndrome) is a congenital developmental disorder of the brain. It ensures that those affected do not produce sex hormones and therefore sexual maturity does not occur. In addition, most KS patients suffer from anosmia, which means that they do not perceive any odors.
The cause of the disease is a genetic change (mutation) that already affects the embryonic development in the womb. In the hormonal control center of the brain (hypothalamus) certain cells are missing that are responsible for the overriding control of sex hormone production in later life. In addition, the gene modification means that the olfactory center in the brain (olfactory bulb) is not or only incompletely developed. Affected people smell nothing or only to a very limited extent.
The disease is named after the German psychiatrist Franz Josef Kallmann, who described it in 1944 as "hypogonadism (lack of sex hormones) and anosmia (lack of sense of smell)". The synonymous term “De Morsier-Kallmann Syndrome” also refers to the Swiss neurologist Georges de Morsier, who also carried out studies on Kallmann syndrome.
Secondary hypogonadism
Kallmann syndrome is a subtype of secondary hypogonadism. This is understood to mean a lack of sex hormones, which is triggered by a malfunction in the hormonal control center in the brain (pituitary gland). The gonads (ovaries, testicles) function normally, but receive little or no signals about the production of sex hormones. If there is anosmia (lack of sense of smell) in addition to the hormone deficiency, doctors speak of Kallmann syndrome.
frequency
Kallmann syndrome is one of the rare diseases; men are more frequently affected than women: On average, around one in 10,000 men and one in 50,000 women get it.
Symptoms
The main symptoms of Kallmann syndrome are a greatly reduced or absent sense of smell and the failure to develop during puberty. How severe the symptoms are varies from patient to patient. If left untreated, both sexes remain sterile.
Missing puberty: Sex hormones are essential for the onset of puberty. If too few or no sex hormones are present, puberty and thus the development of secondary sexual characteristics will not occur.
Symptoms in boys:
- Little or no pubic, armpit and body hair
- Missing beard
- Failure to break his voice
- Micropenis and small testicles: In young men, the penis and testicles fail to develop.
- Undescended testicles (often evident in infancy)
- Tall stature: In healthy people, the growth plates in the long bones close as soon as a certain sex hormone level is reached. If the hormones are missing, those affected grow disproportionately. They are taller than their parents and have long arms and legs.
Symptoms in girls:
In girls, the symptoms are usually less pronounced. Often the only symptom is the absence of the first menstruation (primary amenorrhea), which is why the disease is often recognized late. In contrast to boys, physical development is largely normal despite the illness. For example, the breasts are usually developed normally.
Symptoms in adult male:
Men with Kallmann syndrome typically have reduced bone density (osteoporosis) and muscle mass. Often they have a feminine, external appearance due to a feminine fat distribution. You have erectile dysfunction and you are sterile.
Decreased or absent sense of smell: KS patients do not perceive smells (anosmia) or only perceive smells weakly (hyposmia). This symptom often goes unnoticed because people are used to not smelling anything from birth. The lack of a sense of smell can lead to dangerous situations in individual cases, for example if those affected do not perceive the smell of burning or the smell of spoiled food.
Malformations: Other physical malformations occur less frequently in KS patients. These are, for example, hearing disorders, cleft lip, jaw and palate or missing teeth. Some people are born with only one kidney. Mental development is usually normal in KS.
Osteoporosis: Sex hormones such as testosterone and estrogen play an important role in bone mineralization. If the hormones are missing, the bones are not as stable as in healthy people - the risk of bone fractures increases.
Cause and risk factors
The cause of the Kallmann syndrome is an innate genetic change (mutation).Usually it arises spontaneously, in around 30 percent of cases it is passed on to the offspring from one or both parents.
The genetic change already affects the embryonic development in the womb: the cells for the sense of smell and those responsible for controlling the gonads (ovaries, testes) arise from common progenitor cells.
In Kallmann syndrome, the development of these progenitor cells is disturbed by the gene change. As a result, the cells that are responsible for the overriding control of sex hormone production and the olfactory cells are insufficiently developed. Affected people do not develop puberty and do not perceive any smells.
Sex hormones
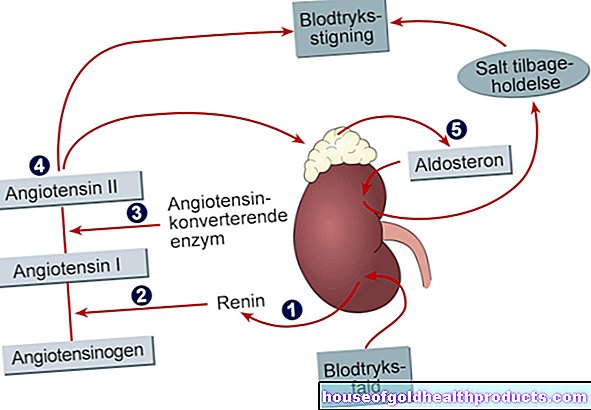
The hypothalamus (a region in the diencephalon) is the body's hormonal control center. In healthy people, the hypothalamus releases the hormone GnRH (gonadotropin-releasing hormone). This in turn stimulates the pituitary gland to release the hormones LH (luteinizing hormone) and FSH (follicle-stimulating hormone).
LH and FSH act on the gonads (ovaries, testes), which ultimately produce the sex hormones: In women, the female sex hormones estrogen and progesterone promote the maturation of the egg cells and trigger ovulation, in men the hormone testosterone causes the formation of sperm.
During puberty, the production of sex hormones begins and with it sexual maturation. If, as in Kallmann syndrome, there is little or no GnRH present, too little or no sex hormones are produced, and puberty does not develop. If left untreated, those affected do not experience sexual maturity and remain sterile.
Risk factors
In most cases, the genetic change occurs spontaneously. How this comes about is not clear. In around 30 percent of all cases, the disease occurs in families: those affected have inherited the mutation from one or both parents.
So far, several mutations have been described that cause Kallmann syndrome. These include the mutations with the names KAL1, FGFR1, FGF8, CHD7, SOX10, PROKR2 and PROK2.
Investigation and diagnosis
The diagnosis of Kallmann syndrome is made late in many cases, as the symptoms often only become apparent in adolescence. This applies especially to boys, in whom the lack of sexual development is usually more clearly visible. In girls, the symptoms are often less pronounced, so that only the absence of the first menstrual period gives rise to a doctor's visit. In addition, in many cases those affected do not suspect an illness behind the symptoms, but rather believe that they are “late-developing”.
In some cases, the disease is already noticeable in infants: Affected boys may have undescended testicles (cryptorchidism) and / or a very small penis (micropenis).
The first point of contact if there are any signs of KS syndrome is the pediatrician, in the case of unwanted childlessness the gynecologist or urologist.
The doctor carries out the following examinations:
Family history: If Kallmann syndrome is suspected, the doctor asks whether there are any known cases of KS in the family.
Physical examination: Underdeveloped secondary sexual characteristics such as a penis that is too small for its age or the absence of the first menstrual period give the doctor the first clues about KS syndrome. He also pays attention to body size, armpit, chest and pubic hair and assesses beard growth.
Smell test: This test is possible from around five years of age. The doctor uses pure fragrances such as vanillin to check whether the patient can perceive the smell.
Blood test: the doctor will determine a changed hormone level with a blood test. Typically the GnRH, LH and FSH levels are decreased or at a low-normal level. The levels of sex hormones in boys and girls in adolescence are pre-pubescent.
Ultrasound examination of the testicles: the doctor uses ultrasound to examine soft tissues such as the testicles.
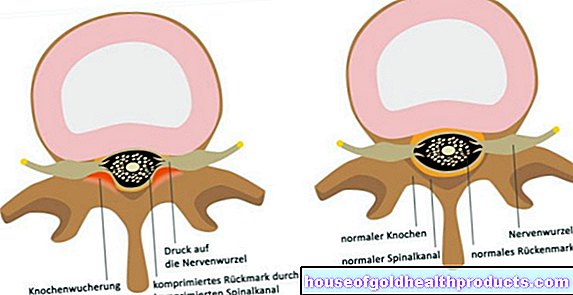
Computed tomography (CT) or magnetic resonance tomography (MRT): With these examination procedures, the doctor checks whether the olfactory center in the brain (olfactory bulb) is developed.
X-ray examination of the hand: With the aid of an X-ray examination of the hand, the doctor determines whether the growth plates are already closed and the body has thus finished growing.
Sperm analysis: The doctor examines whether there are any sperm in the ejaculate.
Genetic test: The genetic test is used to determine the exact mutation that is causing the disease.
How is Kallmann syndrome treated?
Kallmann syndrome is easily treatable. Those affected receive replacement treatment with sex hormones. If the disease is recognized and treated before puberty, those affected usually lead a largely unrestricted life. This includes regular puberty development and a normal sex life.
Sex hormone administration: Men receive testosterone, women estrogens and progesterone. The hormone preparations are available in the form of injections, gels or patches. Hormone therapy is usually continued for life in men and until menopause in women.
In 10 to 20 percent of cases, a congenital GnRH deficiency resolves after hormone replacement therapy has ended. Following therapy, the patients have normal hormone levels and experience normal sexual maturity. For this reason, doctors recommend pausing therapy every one to two years to determine the need to continue therapy.
Giving sex hormones if you want to have children: the body needs GnRH in order for sperm to be formed. For this reason, men who want to father a child are given the hormone GnRH instead of testosterone. It takes 18 to 24 months for sperm production to begin. In about 80 percent of the cases, men are fertile afterwards. Men with undescended testicles have a slightly less favorable prognosis.
Treatment of osteoporosis: patients with reduced bone density receive calcium and vitamin D. In addition, sport and exercise are recommended to strengthen the bones.
Anosmia: There is currently no therapy to restore the sense of smell.
Psychotherapy: For some KS patients, the disease is a serious psychological burden. The psychotherapist is the right contact here.
Course of the disease and prognosis
How the Kallmann syndrome progresses varies from person to person. The symptoms vary from patient to patient. It is possible that the disease is already noticed in infancy, diagnosed in adolescence, or the hormone deficiency only appears in adulthood.
If the disease is diagnosed in good time, the prognosis is very good. Sexual maturation is achieved in all patients with appropriate hormonal treatment. The patients experience a regular development of puberty, are fertile and have a normal life expectancy. Almost all patients who wish to have children become fertile with appropriate treatment.
If KS is only recognized and treated after the age of 16, it may already have grown tall. This change cannot be reversed even with medication.
Prevent
Since it is a genetic disease, no prevention is possible.
Tags: menshealth home remedies pregnancy birth