stupor
Martina Feichter studied biology with an elective subject pharmacy in Innsbruck and also immersed herself in the world of medicinal plants. From there it was not far to other medical topics that still captivate her to this day. She trained as a journalist at the Axel Springer Academy in Hamburg and has been working for since 2007 - first as an editor and since 2012 as a freelance writer.
More about the experts All content is checked by medical journalists.
Stupor is a state of mental and motor paralysis. Although those affected are awake, they hardly or not at all react to external stimuli. They are motionless, sometimes their muscles are tense. They are often silent or clearly restricted in their linguistic communication. Read here how stupor manifests itself, what triggers it and what can be done about it.

Brief overview
- What is stupor? State of psychomotric paralysis. Affected people do not react to their environment, although they are neither sleeping nor are their consciousness disturbed.
- Causes: e.g. B. Depression, schizophrenic psychosis, organic reasons (e.g. encephalitis, brain tumor, liver disease, dementia), medication or poisoning
- Symptoms: i.a. Loss of reaction, inability to speak, cramped muscles, impaired vision
- When to the doctor Always - In the vast majority of cases, stupor is a sign of severe physical or mental illness.
- Examinations: taking the medical history (anamnesis), physical examination, laboratory examinations, neurological examination, measurement of brain waves (EEG), imaging procedures (such as MRI)
- Treatment: depending on the cause, e.g. treatment of the underlying disease, administration of antidepressants or neuroleptics, electroconvulsion therapy. Also important: constant attention, addressing and touch - also if the patient does not react.
Stupor: definition
The term stupor comes from Latin and means something like "solidification". Correspondingly, the drive is extremely reduced in a stupor, those affected do not react at all or only minimally to environmental stimuli. Nevertheless, they perceive their environment and what is going on in it, even with particular sensitivity - they just cannot participate in it or react to it.
For example, those affected do not turn their heads or gaze to other people who come up to them or who touch them. They have fallen silent (medical mutism) or at least are severely restricted in their linguistic communication. Contacting those affected is therefore only possible to a very limited extent or not at all. Some patients also have a high fever.
Difference Between Stupor and Catatonia
At first glance, both terms appear synonymous, as they denote physical rigidity. Still, stupor and catatonia are different.
As early as the 1860s, the psychiatrist Ludwig Kahlbaum described catatonia as "motor-muscular or mental tension" which, according to his definition, takes a course that cyclically consists of the successive symptoms of moodiness, mania, stupor, confusion and possibly dementia and delusions consists.
Seen in this way, catatonia is an umbrella term for extremely high muscle tone all over the body, stupor is a sub-category or a single catatonic symptom.
Stupor: causes and possible diseases
Stuporous states can have a wide variety of causes, which can be subdivided as follows.
Depressed stupor
It is the result of extreme inhibition of drive in people with severe depression. Those affected appear resigned and less autistic than in the catatonic form. Although the drive is strongly inhibited, there is a risk of suicide. The patients must therefore be monitored.
Catatonic stupor
A catatonic stupor occurs in the context of a schizophrenic psychosis. The muscle tension (muscle tone) of those affected is greatly increased (rigor = muscle rigidity). This can lead to catalepsy, a "waxy flexibility": The patient maintains postures that are passively induced by other people, such as the doctor (such as strong curvature of the arms and fingers) in a way that would never be arbitrarily possible - and sometimes this overtime.
Psychogenic (dissociative) stupor
This term includes all those cases of stupor that occur without depression or schizophrenic psychosis. There is also no evidence of an organic cause. Rather, a close connection to a recent traumatic experience or a stressful problem can be seen.
Organically caused stupor
If a patient is stuporous, it can also have organic causes such as:
- Inflammation of the brain or meninges (encephalitis, meningitis)
- Brain edema
- Seizure disorders
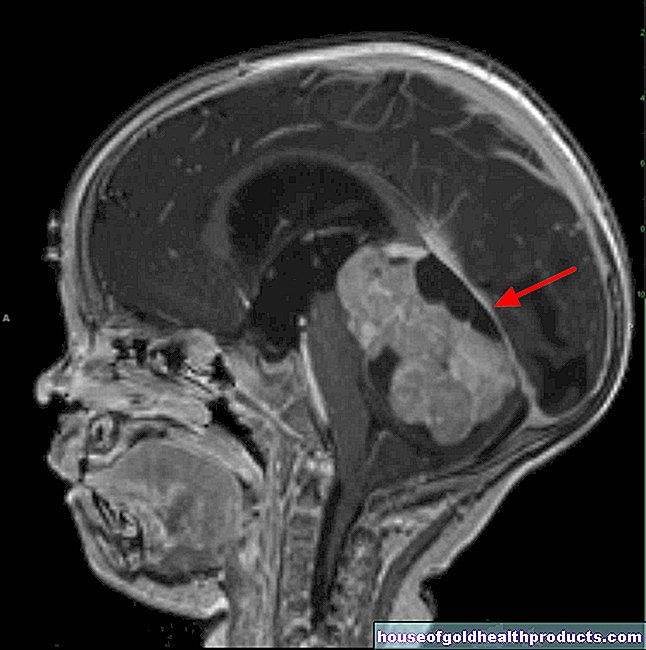
- Space-consuming processes in the brain (tumor, etc.)
- dementia
- Liver disease
- Addison's disease (underactive adrenal cortex)
- high potassium levels (hyperkalemia)
- Porphyria (a metabolic disorder)
Drug / toxic stupor
Stupor can occur, for example, in the context of neuroleptic malignant syndrome (NMS) - a very rare but life-threatening side effect of neuroleptics. These are drugs that are given, for example, for delusions, schizophrenia or severe states of excitement.
Poisoning (intoxication) with neuroleptics or with drugs such as PCP ("Angel Dust") or LSD can lead to stupor.
Stupor: symptoms
Probably the most obvious symptom of a stupor is that the person concerned shows no reaction to external stimuli. In addition, a stupor - depending on the cause - sometimes expresses itself with other signs:
- Signs in the area of the muscles: The person concerned is unable to move, the muscles are tense - sometimes so strong that they pull the head back, stretch the arms or legs of the person concerned. Sometimes involuntary muscle contractions also occur.
- Signs around the eyes: The pupil in one or both eyes may be dilated (dilated) or rigid. The eyes may not move at all, limited or abnormal.
- no speaking: those affected cannot speak. Doctors also call this phenomenon mutism.
- Other symptoms: Sometimes with a stupor there are also symptoms that are not attributable to the solidification itself, but to the disease causing it. For example, meningitis can be accompanied by vomiting, fever, headache and stiff neck.
Stupor: complications
A serious complication with a stupor is that striated muscle fibers dissolve or disintegrate (rhabdomyolysis). Such muscle fibers are mainly found in the skeletal muscles. The large amount of muscle protein (myoglobin) released during the breakdown can lead to acute kidney failure.
Other possible complications are:
- Pneumonia with "blood poisoning" (sepsis)
- Thrombosis of the leg veins
- Skin sores (ulcers) caused by bedsores (bedsores)
- Disorders of the water and salt (electrolyte) balance
The longer the stupor persists, the more likely such complications are and the higher the patient mortality.
Stupor: When should you see a doctor?
A stupor is usually the result of a mental shock, a serious mental or physical illness. Those affected always need medical treatment!
Stupor: What is the doctor doing?
The doctor must first determine whether it is actually a stupor and what is causing it. Then he can initiate appropriate therapy.
Stupor: diagnosis
The doctor will first take the patient's medical history (anamnesis). Usually this is done in conversation. Often, however, communication with the person concerned is not possible. Then relatives can provide valuable information. In the anamnesis interview, the doctor specifically asks about previous psychiatric illnesses (such as depression, schizophrenic psychosis).
This is followed by a physical examination. For example, the doctor checks the muscle tone and whether the patient is responding to pain stimuli or speech.
Laboratory examinations (blood, cerebrospinal fluid = cerebrospinal fluid), measurement of electrical brain waves (EEG), neurological examinations and imaging procedures (such as magnetic resonance imaging) can provide further important information. They can help identify the exact cause of stupor and rule out other causes of the symptoms that are present.
Stupor: treatment
Treatment depends on the cause of the stupor:
In the case of organically caused stupor, the underlying disease (such as cerebral edema, encephalitis) is primarily treated.
Patients with catatonic stupor receive neuroleptics (antipsychotics) such as haloperidol or fluphenazine. The doctor may also prescribe lorazepam (sedative and anxiety reliever). He can also try the latter in the case of psychogenic stupor.
Patients with depressed stupor are given antidepressants such as doxepin, clomipramine, amitriptyline or citalopram. Neuroleptics are also used.
In some cases of stupor, electroconvulsive therapy (electroconvulsive therapy, ECT) may be necessary: Under short anesthesia, the patient receives electrical impulses that trigger a generalized seizure. The procedure is considered to be low-risk and is usually repeated on several consecutive days. Before starting treatment, it is necessary to discontinue any neuroleptics and antidepressants that may be given.
Other measures
With Stupor it is also important that all persons involved in the treatment give constant attention - despite the patient's indifference. This also includes addressing them regularly, even if the patient does not speak or hardly speaks at all. According to the testimony of former stupor patients, this can have a confidence-building and relieving effect.
A calm, low-stimulus atmosphere is very important, especially in the case of psychogenic stupor. Often only then is a therapeutic conversation possible.
The patients receive all-round surveillance (possibly seated guard) with control of the vital functions and measures to prevent blood clots (thrombosis) and bedsores (bedsores). Patients who refuse to eat are artificially fed.
Treatment in the intensive care unit is necessary if complications occur (e.g. muscle breakdown = rhabdomyolysis, high fever, increased inflammation in the blood, pneumonia, sepsis). Even if the diagnosis is uncertain, (potential) stupor patients should receive intensive medical treatment.
Stupor: You can do that yourself
Even if patients are unresponsive, it is important to be aware that they are awake. Appropriate behavior with friendly speech and touch can support the healing process and calm and relieve stupor patients.
Tags: womenshealth prevention Diseases