Dilated cardiomyopathy
Marian Grosser studied human medicine in Munich. In addition, the doctor, who was interested in many things, dared to make some exciting detours: studying philosophy and art history, working on the radio and, finally, also for a Netdoctor.
More about the experts All content is checked by medical journalists.Dilated cardiomyopathy is a special form of heart muscle disease. The left ventricle in particular expands. Those affected suffer from arrhythmias and symptoms of cardiac insufficiency. Genetic changes and various environmental factors can be considered as causes. The disease can usually not be cured, but the symptoms can be alleviated. Read everything about dilated cardiomyopathy here!
ICD codes for this disease: ICD codes are internationally recognized codes for medical diagnoses. They can be found, for example, in doctor's letters or on certificates of incapacity for work. I43I42
Dilated cardiomyopathy: description
Dilated cardiomyopathy (DCM) is a serious disease in which the heart muscles change their structure. It no longer works properly and thus the heart pumps less blood into the body's circulation during the expulsion phase (systole). In addition, the heart muscle can usually no longer relax properly, so that the phase in which the heart chambers fill with blood (diastole) and expand is also disturbed.
This form of cardiomyopathy got its name because the left heart chamber in particular dilates, i.e. expands, in the disease. As the disease progresses, the right ventricle and atria can also be affected. The heart walls can become thinner as they expand.
Who does dilated cardiomyopathy affect?
Dilated cardiomyopathy is the most common cardiomyopathy. In about 50 percent of cases, the cause of the disease cannot be determined (primary or idiopathic DCM). The other dilated cardiomyopathies are the result or the end state of various diseases and harmful environmental factors (secondary DCM). Idiopathic DCM is diagnosed in around 6 out of 100,000 people in Germany every year. Most patients are between 20 and 40 years old at diagnosis, with men about twice as likely to be affected as women.
Dilated cardiomyopathy: symptoms
Patients with DCM often have the typical symptoms of heart failure (heart failure). On the one hand, because of its limited performance, the heart does not manage to supply the body with sufficient blood and thus also with oxygen (cyanosis) - doctors speak of forward failure.
On the other hand, heart failure is often associated with backward failure. This means that the blood accumulates in the blood vessels that lead to the heart. If the left heart is affected (left heart failure), such a congestion of blood mainly affects the lungs. If the right ventricle is weakened, the blood builds up in the venous vessels that come from all over the body.
Dilated cardiomyopathy is initially noticeable with the symptoms of progressive left heart failure. The patients suffer from:
- Fatigue and decreased performance. Those affected often complain of a general feeling of weakness.
- Difficulty breathing during physical exertion (exertional dyspnea). If the cardiomyopathy is already very advanced, difficulty breathing can occur even at rest (resting dyspnea).
- Fluid build-up in (pulmonary edema) and around the lung tissue (pleural effusion), which can exacerbate shortness of breath. You may notice pulmonary edema from rattling noises when breathing.
- Chest tightness (angina). This feeling also appears mainly during physical exertion.
In the course of the disease, dilated cardiomyopathy often affects the right ventricle as well. In such cases, doctors speak of global insufficiency. In addition to the symptoms of left heart failure, patients then complain of fluid retention (edema), especially in the legs. In addition, the neck veins often protrude because blood also builds up from the head and neck.
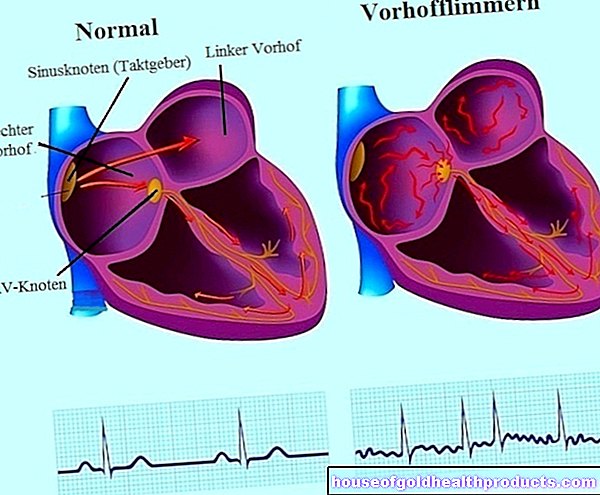
Since the structure of the heart muscle changes in a DCM, the generation and transmission of electrical stimuli to the heart is also disturbed. Therefore, dilated cardiomyopathy is often associated with cardiac arrhythmias. Those affected occasionally feel this as a heart stumble (palpitations). As the disease progresses, the arrhythmias can become more dangerous and cause circulatory collapse or - in the worst case - even sudden cardiac death.
The left ventricle in particular dilates in dilated cardiomyopathy. This in turn pulls the fiber ring to which the mitral valve is attached apart. As the DCM progresses, there is a risk of mitral regurgitation.
Because of the disturbed blood flow in the auricles and chambers of the heart, blood clots form more easily in dilated cardiomyopathy than in healthy people. If such a clot loosens, it can enter the arteries with the bloodstream and block them. This can lead to serious complications such as a pulmonary infarction or stroke.
Dilated cardiomyopathy: causes and risk factors
Dilated cardiomyopathy can be primary or secondary. Primary means that it arises directly in the heart muscle and is limited to this. In secondary forms, other diseases or external influences are the triggers of DCM. The heart or other organs are then only damaged as a result of these factors.
Primary dilated cardiomyopathy is genetic in some cases. In a good quarter of the illnesses, other family members are also affected. The triggers of primary DCM are often unknown (idiopathic, about 50 percent).
Dilated cardiomyopathy is a type of heart muscle disease that is relatively often secondary. Examples of triggers include:
- Longstanding, excessive alcohol and drug use (such as cocaine). Above all, alcohol abuse is considered to be one of the main risk factors for dilated cardiomyopathy.
- Inflammation of the heart muscle (myocarditis), for example caused by viruses or bacteria (examples: Chagas disease, Lyme borreliosis).
- Valvular heart disease
- Autoimmune diseases such as systemic lupus erythematosus (SLE).
- Hormonal disorders (especially growth and thyroid hormones)
- Medication: Certain cancer drugs (cytostatics) can cause dilated heart muscle disease as a rare side effect.
- Malnutrition
- Radiation therapy in the chest area
- Congenital diseases that affect the protein build-up in muscles, e.g. muscular dystrophies.
- Environmental toxins: Heavy metals in particular, such as lead or mercury, accumulate in the heart muscle and disrupt the cell metabolism.
- Coronary heart disease (CHD). In those affected, the heart muscle constantly receives too little oxygen and therefore changes its structure (ischemic cardiomyopathy). A narrowing of the coronary arteries is to blame.
- In very rare cases, dilated cardiomyopathy occurs during pregnancy. However, the connections are still unclear here.
According to more recent definitions, cardiomyopathies only include cardiomyopathies that are not a direct result of other cardiovascular diseases. Accordingly, ischemic cardiomyopathy is not one of the dilated cardiomyopathies. However, in some textbooks they are still considered to be secondary DCM.
Dilated cardiomyopathy: examinations and diagnosis
First, the doctor asks the patient about their medical history (anamnesis). He is particularly interested in what symptoms the patient has, when they occur and how long they have existed. It is also important whether the patient drinks a lot of alcohol, takes other drugs or already has previous illnesses.
The conversation is followed by a physical examination. Doctors can see some signs of heart failure with the naked eye. For example, the skin of those affected often appears bluish due to the chronic lack of oxygen (cyanosis). Pulmonary edema may be noticed as a rattle noise when listening to the lungs.
Many heart muscle diseases show similar symptoms. In order to be able to determine exactly which type of cardiomyopathy is present, special diagnostics and the support of medical devices are required. The most important investigations are:
- Cardiac ultrasound (echocardiography): In DCM, the enlarged left heart is particularly noticeable. The heart walls may be thinner than normal and move irregularly. Especially in the case of advanced dilated cardiomyopathy, the doctor measures a reduced ejection rate (ejection fraction, EF).
- Electrocardiogram (EKG): Many DCM patients have a special disturbance of the electrical heart activity on the EKG, which is known as left bundle branch block.
- Chest x-ray: Because of the enlarged left ventricle, the heart appears enlarged on x-rays (cardiomegaly). Pulmonary congestion can also be recognized by it.
- Cardiac catheterization. As part of this method, the coronary arteries can be examined (coronary angiography) and tissue samples can be taken from the heart muscle (myocardial biopsy). The tissue examination under the microscope enables a reliable diagnosis.
There are also certain blood values that can be increased in connection with DCM. However, these findings are hardly specific, but occur in many cardiac and other diseases. For example, high levels of BNP generally indicate cardiac insufficiency.
Dilated cardiomyopathy: treatment
Whenever possible, attempts are made to treat the cause of dilated cardiomyopathy. For example, bacteria are combated if they are the cause of heart inflammation, or possible hormonal imbalances are compensated. If alcohol or drugs are responsible for DCM, it is important that the patient avoid these harmful substances.
If the cause is unknown and / or cannot be treated, then only symptomatic treatment of the DCM is possible. The priority then is to alleviate the symptoms of heart failure and delay their progress as much as possible. Various groups of drugs such as beta blockers, ACE inhibitors and diuretics are available for this. "Blood-thinning" drugs are designed to prevent blood clots from forming.
Basically, patients with dilated cardiomyopathy should take it easy in order not to overwhelm the weak heart. However, "dosed training" has advantages over complete immobilization.
In the case of advanced DCM, it makes sense to insert a defibrillator into the patient (ICD implantation). This can prevent massive arrhythmias from leading to sudden cardiac death. If the heart is severely damaged, the dilated cardiomyopathy progresses quickly despite treatment and there is no other way of helping the patient, the last possible treatment option is a heart transplant. DCM is the most common reason for heart surgery to be "transplanted".
Dilated cardiomyopathy: disease course and prognosis
The prognosis for the disease is unfavorable for dilated cardiomyopathy. Life expectancy and the course of the disease ultimately depend on the degree of cardiac insufficiency. Appropriate medication can support the heart, but cannot stop or even reverse the progression of the disease. A DCM restricts the everyday life of those affected more and more.
80 to 90 percent of patients with DCM die within the first ten years of diagnosis. Often the consequences of heart failure or sudden cardiac death are the cause.
The patients themselves can hardly influence the course of the disease. But those who do without drugs and only drink alcohol in moderation avoid at least two risk factors for dilated cardiomyopathy.
Tags: sleep prevention magazine










.jpg)