Polycythemia vera
Astrid Leitner studied veterinary medicine in Vienna. After ten years in veterinary practice and the birth of her daughter, she switched - more by chance - to medical journalism. It quickly became clear that her interest in medical topics and her love of writing were the perfect combination for her. Astrid Leitner lives with daughter, dog and cat in Vienna and Upper Austria.
More about the experts All content is checked by medical journalists.Polycythemia vera (PV) is a rare, slowly progressing form of blood cancer. There is an uncontrolled increase in blood cells, causing the blood to thicken. The result: the risk of blood clots (thrombosis) increases. Read here which complaints arise and how PV is treated.
ICD codes for this disease: ICD codes are internationally recognized codes for medical diagnoses. They can be found, for example, in doctor's letters or on certificates of incapacity for work. D45

Brief overview:
- What is polycythemia vera? Rare disease of the blood-forming cells of the bone marrow, form of blood cancer
- Prognosis: If left untreated, the prognosis is unfavorable; with treatment, the median survival time is 14 to 19 years.
- Treatment: bloodletting, medication (blood thinners, cytostatics, JAK inhibitors), bone marrow transplantation, prevention of thrombosis
- Symptoms: fatigue, night sweats, itching, bone pain, weight loss, thrombosis
- Causes: Acquired genetic modification (mutation)
- Risk factors: old age, previous thrombosis
- Diagnostics: blood tests, molecular genetic tests for a genetic change, bone marrow biopsy, ultrasound
- Prevention: Healthy lifestyle, examination for genetic changes in familial accumulation
What is PV?
Polycythemia vera (polycythemia vera, PV) is a rare chronic disease of the blood-forming cells of the bone marrow. Since the cells multiply in an uncontrolled manner, it is a form of blood cancer: Doctors also speak of "primary polycythemia" or "Vaquez-Osler disease" or "Vaquez-Osler disease". PV belongs to the group of "myeloproliferative neoplasias" (MPN), a group of rare, malignant diseases of the bone marrow.
The term polycythemia (also: polycythemia) basically means an increase in the number of red blood cells (erythrocytes), hematocrit (proportion of solid blood components) and hemoglobin (red blood pigment). Depending on the cause, a distinction is made between different forms of polycythemia:
- Primary polycythemia: polycythemia vera (PV)
- Secondary polycythemia: through increased production of erythropoietin (a hormone that promotes the formation of red blood cells in the bone marrow, known as erythropoiesis)
- Relative polycythemia: due to a lack of fluid in the body, such as severe vomiting
During PV, it is mainly red and white blood cells that multiply in an uncontrolled manner, and to a lesser extent the blood platelets as well. A special form of PV is polycythemia vera rubra, in which only the red blood cells multiply. However, it occurs much less frequently compared to the PV.
PV increases the risk of blood clots and thrombosis. The increased proportion of blood cells (hematocrit) makes the blood thicker, which increases the risk of thrombosis. In the worst case, the internal organs are no longer adequately supplied with blood. This can lead to complications such as heart attacks and strokes. Blood clots in the veins (e.g. deep vein thrombosis) are not only painful, but sometimes cause a pulmonary embolism if they loosen and are washed into the lungs with the blood.
Course of Primary
A PV is insidious and in many cases does not trigger any symptoms at the beginning. There are two phases of the disease:
Chronic phase (polycythemic phase): The increased production of red blood cells can last up to 20 years unnoticed.
Progressive late phase (spent phase): In up to 25 percent of patients, a "secondary myelofibrosis" develops from the PV. Blood formation then no longer takes place in the bone marrow, but in the spleen or liver. In around ten percent of cases, PV changes into myelodysplasia (myelodysplastic syndrome, MDS) or acute myeloid leukemia (AML).
frequency
PV is a rare disease: every year between 0.4 and 2.8 percent of the population across Europe develop it, women about as often as men. At the time of diagnosis, those affected are on average between 60 and 65 years old.
PV and disability
Some patients feel good despite their illness and are fully able to work. Others are faced with the massive effects of polycythemia vera. If severe symptoms persist, it is advisable to submit an application to determine whether the person is severely disabled.
You can get information as well as the applications for the determination of the severe disability in the respective municipality or city administration as well as at the health authorities!
What is my life expectancy with PV?
The prognosis for PV varies from case to case. If left untreated, survival time is very short, averaging 1.5 years. Patients who are treated have a significantly better life expectancy with an average of 14 to 19 years. The prevention of vascular occlusions (thromboembolism) and myelofibrosis as well as acute leukemia, which are considered to be the most common causes of death, is of particular importance here.
How is Primary Treated?
The doctor decides which treatment of polycythemia vera is the best in the individual case, depending on the course of the disease and the patient's condition. The primary goals of treatment are to relieve the symptoms and to prevent thrombosis and the progression of the disease. Possible secondary diseases of PV are myelofibrosis and acute myeloid leukemia.
It is essential for the treatment that the patient has regular check-ups with the doctor. The doctor repeatedly draws blood and adapts the treatment to the respective situation of the patient. Therefore, it is common for the doctor to modify the ongoing therapy several times.
Lowering the risk of thrombosis
General measures to reduce the risk of blood clots include:
- Weight normalization
- Regular exercise
- Adequate hydration
- Avoid long periods of sitting
- Treatment of existing cardiovascular diseases
- Wearing compression stockings on long (air) trips
Lowering the hematocrit
Bloodletting is the quickest and easiest way to lower the hematocrit level. To do this, the doctor initially takes 250 to 500 ml of blood from the patient every two to three days until the proportion of red blood cells in the blood (in both sexes) has fallen below 45 percent. In the further course, the time interval and the amount of blood drawn are adapted to the respective hematocrit value of the patient. The aim is to keep the hematocrit level permanently below 45 percent.
As an alternative to bloodletting, the doctor uses what is known as "erythrocytapheresis". This procedure is similar to dialysis (blood washing in case of kidney diseases): The blood is not freed of toxins, but of red blood cells (erythrocytes).
Medication
- Anticoagulants (antiplatelet agents) such as acetylsalicylic acid prevent platelets from clumping together and blood clots from forming.
- So-called cytostatics (cell poisons) reduce the greatly increased number of cells by inhibiting the formation of new blood cells in the bone marrow. Alternatively, hormone-like messenger substances such as interferon-alpha can also be used.
- According to the latest findings, so-called JAK inhibitors are particularly suitable for the therapy of PV. They inhibit the activity of certain substances that cause too many blood cells to be formed.
Stem cell transplant
Stem cell transplantation is the only treatment that can cure PV. However, due to its risk of severe side effects, it is only suitable for patients in the advanced stages of the disease. It takes the form of an infusion in which the diseased bone marrow is replaced with healthy marrow from a suitable donor. Before doing this, however, all of the patient's diseased bone marrow cells must be killed by means of strong chemotherapy and radiation.
After the transplant, the patient is given drugs that prevent the new immune system, which was also transmitted by the donor, from attacking the recipient's body. During this time, the patient is particularly susceptible to infections. It takes about half a year for the new immune system to adapt to the body. Once this phase has been overcome, the limitations in the life of those affected usually gradually disappear.
What can i do on my own?
These tips will help alleviate the typical symptoms of PV:
Fatigue: Most PV patients experience severe exhaustion and fatigue. It cannot be prevented, but under certain circumstances "managed": Pay attention to when you feel particularly tired. Plan your activities to come when you usually feel best. Physical activity also counteracts fatigue and improves your sleep.
Itching: Taking a lukewarm bath with a little baking soda or uncooked oatmeal before bed will relieve itching. Use mild soap with no dyes and rinse well, then nourish your skin with a rich moisturizer.
Night sweats: Light, loose-fitting clothing and cotton bed linen make you sweat less. Have a towel and glass of water ready, and try not to eat anything heavy before you go to bed.
Diet: Diet plays an important role, especially with chronic diseases. The physical and psychological functions are only maintained when the energy and nutrient requirements are met. There is no special diet to favorably influence PV.
If there are no intolerances or allergies, a diet that is also beneficial to healthy people is advisable. We recommend a Mediterranean diet, which is considered to be good and balanced in its composition, as it uses a lot of vegetables, fish and high-quality vegetable oils instead of animal fats.
General recommendations for a balanced diet:
- Eat a variety of foods, especially plant-based foods.
- Eat fruits and vegetables daily: Up to three servings of vegetables a day, including legumes and nuts.
- Give preference to whole grain products, especially bread, pasta, rice and flour.
- Only eat small amounts of animal-based foods: fish once or twice, meat no more than 300 to 600 g per week.
- Avoid hidden fats, prefer vegetable oils such as rapeseed or olive oil.
- Use salt and sugar very sparingly.
- Drink enough water - around 1.5 liters per day.
- Avoid sugary and alcoholic drinks.
- Prepare your meals gently - cook food for as long as necessary and as short as possible.
- Take your time to eat.
- Watch your weight and keep moving.
Symptoms
The symptoms of polycythemia vera vary from person to person and largely depend on the stage of the disease. Many patients have no symptoms at all, especially at the beginning of the disease. Precisely because the diagnosis is often only made by chance and those affected are completely symptom-free at the time of diagnosis, knowledge of the disease is initially a shock for many.
The disease always begins insidiously, the symptoms progress only slowly. Signs of PV can include:
- Tiredness, exhaustion
- Reddened facial skin, blue-red skin and mucous membranes, high blood pressure (caused by the "thickened" blood)
- Itching, especially when the skin is moistened with water (affects 70 percent of patients)
- Night sweats and excessive daytime sweating
- Bone pain
- Weight loss that is neither wanted nor due to other diseases
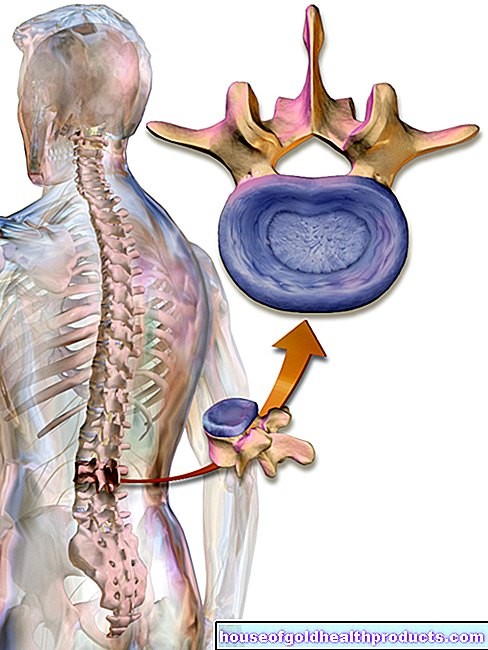
- Abdominal pain (diffuse pain in the right upper abdomen) and a feeling of fullness due to enlargement of the spleen (splenomegaly). Because of the increased cell production, the spleen has to break down a particularly large number of old and changed blood cells. In addition, in a later phase of the disease, the formation of blood cells shifts to the spleen.
- Circulatory disorders in the hands and feet, visual disturbances, discomfort or tingling in the arms and legs (caused by blockages in smaller blood vessels)
- Stroke, heart attack, deep vein thrombosis (due to blockages in larger blood vessels)
What are the causes of PV?
PV is caused by a malfunction of the blood-forming cells in the bone marrow. This is triggered by a genetic change (mutation) that can be detected in almost all patients with polycythemia vera.
97 percent of all PV patients have a mutation in the so-called JAK gene (abbreviation for “Janus Kinase 2”). It causes the blood-forming cells to multiply in an uncontrolled manner. Too many blood cells are produced, especially red and white blood cells. Platelets may also be excessively produced and “thicken” the blood. The consequence is an increased risk of thrombosis.
Even if the PV occurs more frequently in some families, it is not a classic hereditary disease: The genetic change is not passed on, but only develops in the course of life. How this comes about is unknown.
What does the doctor?
Since polycythemia vera usually does not cause any symptoms in the early stages, the suspicion of PV often only arises as an incidental finding during routine blood tests. It is noticeable that the number of red blood cells and the hematocrit are significantly increased. Another indication is increased platelet and leukocyte counts.
If these blood values are elevated, the family doctor usually refers the patient to a doctor (hematologist) who specializes in blood disorders for further clarification.
This makes the diagnosis of PV based on three criteria:
Blood values: Typical for PV are increased values of the blood-forming cells and of the hematocrit. The normal value of the hematocrit is 37 to 45 percent for women and 40 to 52 percent for men. At the time of diagnosis, PV patients often have values above 60 percent.
JAK2 mutation: Using molecular genetic methods, the blood is examined for genetic changes (mutations).
Special features in the bone marrow: In order to be able to examine the bone marrow for typical changes, the doctor takes a small amount of bone marrow from the patient under local or short anesthesia.
Vascular changes or existing blood clots as well as the spleen that is typically enlarged in PV can be diagnosed with the help of an ultrasound examination, among other things.
Prevent
Since the cause of the genetic change that causes the disease is unknown, there are no recommendations to prevent PV. If polycythemia vera occurs more frequently in a family, genetic counseling is recommended. A specially trained doctor uses a blood test to determine whether someone has the mutation in the JAK gene.
If the corresponding genetic change is detected, this does not necessarily mean that the PV actually breaks out!
Tags: stress eyes sports fitness