Diaphragmatic hernia
Florian Tiefenböck studied human medicine at the LMU Munich. In March 2014, he joined as a student and has supported the editorial team with medical articles ever since. After receiving his medical license and practical work in internal medicine at the University Hospital Augsburg, he has been a permanent member of the team since December 2019 and, among other things, ensures the medical quality of the tools.
More posts by Florian Tiefenböck All content is checked by medical journalists.The diaphragmatic hernia (medical: hiatal hernia) occurs when there is a defect or weakness in the diaphragm. As a result, portions of the stomach or abdominal contents of different sizes can pass into the chest cavity. A diaphragmatic hernia usually only needs to be operated on if there are complaints. Find out everything you need to know about the diaphragmatic hernia here.
ICD codes for this disease: ICD codes are internationally recognized codes for medical diagnoses. They can be found, for example, in doctor's letters or on certificates of incapacity for work. K44

Diaphragmatic hernia: description
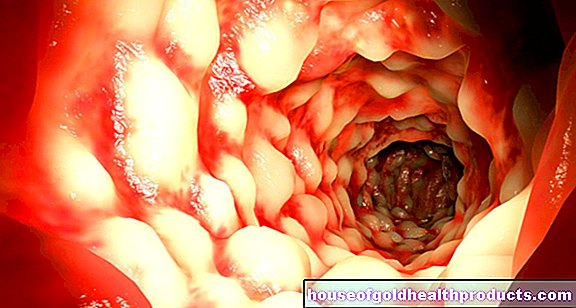
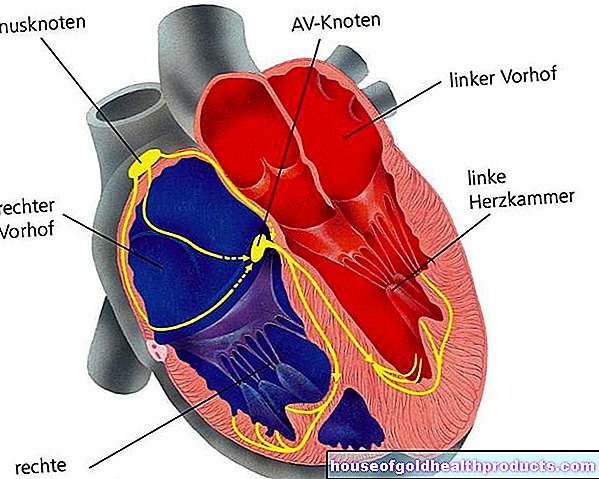
In the case of a diaphragmatic hernia, known medically as a hiatal hernia, parts of the abdominal organs shift through an opening in the diaphragm into the chest (thorax). The dome-shaped diaphragm is made up of muscle and tendon tissue. It separates the thoracic from the abdominal cavity. It is also considered to be the most important respiratory muscle. It has three large openings: In front of the spine is the so-called aortic slit through which the main artery (aorta) and a large lymphatic vessel pass. The main artery runs behind the abdomen and its organs. The inferior vena cava runs through the second larger opening - it is firmly attached to the surrounding tendon tissue of the diaphragm.
The esophagus passes through the third large hole, the esophageal hiatus, where it joins the stomach just below the diaphragm. The esophageal opening forms a direct connection between the chest and the abdomen. Since the muscle tissue is relatively loose at this point, a diaphragmatic hernia can occur here in particular.
Hiatal hernias are subdivided according to the origin and location of the parts that protrude into the chest cavity.
|
Type I hernia |
= axial hiatal hernia The gastric entrance (cardia), where the esophagus merges into the stomach, shifts vertically upwards (more precisely along the longitudinal axis of the esophagus) through the opening. It then lies over the diaphragm. This diaphragmatic hernia often affects the entire upper part of the stomach, the fundus of the stomach. |
|
Type II hernia |
= paraesophageal hiatal hernia A portion of the stomach of different sizes passes next to the esophagus into the chest cavity. In contrast to the type I hernia, the entrance to the stomach remains below the diaphragm. |
|
Type III hernia |
This diaphragmatic hernia is a hybrid of types I and II. It usually begins with an axial hiatal hernia. Over time, more and more stomach sections shift to the sides of the esophagus into the chest cavity. The extreme form of this hiatal hernia is the so-called "upside-down stomach": the stomach lies completely in the chest. |
|
Type IV hernia
|
This is a very large diaphragmatic hernia in which other abdominal organs such as the spleen or large intestine also enter the chest cavity. |
Extrahiatal diaphragmatic hernias
The popular term diaphragmatic hernia usually means the organ displacement through the esophageal slit (hiatus oesophageus), which is why it is also called a hiatal hernia. In addition, there are also diaphragmatic hernias in which organs of the abdominal cavity pass through other openings in the diaphragm. These are summarized under the term extraiatal (i.e. outside the esophageal slit) diaphragmatic hernias. For example, there is a hole (Morgagni) at the connection point to the sternum, through which loops of intestine are preferentially displaced (Morgagni hernia, parasternal hernia). And a triangular gap in the back of the muscular diaphragm (Bochdalek gap) can also cause a hernia.
frequency
The diaphragmatic hernia through the esophageal slit is by far the most common form. Axial hernias are found in approximately 90 percent of these cases. In contrast, fractures to the side of the esophagus, the paraesophageal hernias, occur very rarely alone. They are usually found in mixed forms (type III hernias). Diaphragmatic hernias are more common in older people. If the hernia arises due to an incorrectly developed diaphragm, then it is the congenital form. Doctors find a diaphragmatic defect in around two to five in 10,000 births. Most can be found on the left (80-90 percent).
According to federal health reports, a good 10,000 diaphragmatic hernias were diagnosed in German hospitals in 2012. Women were affected roughly twice as often as men. Congenital diaphragmatic hernias were found in 237 newborns in the same year.
Diaphragmatic hernia: symptoms
Whether you have symptoms with a diaphragmatic hernia usually depends on the type and extent of the respective hernia.
Axial hiatal hernia
With type I diaphragmatic hernia, there are usually no symptoms. Patients often report heartburn and pain behind the breastbone or in the upper abdomen. But it is less a question of diaphragmatic hernia complaints; rather, the symptoms are due to an accompanying reflux disease. The contents of the stomach, especially the acidic gastric juice, flow into the esophagus. Normally, a closing mechanism prevents this reflux: Muscles at the entrance to the stomach (lower esophageal sphincter) tighten and thus protect the esophagus from stomach acid. In addition, the esophagus flows very steeply into the stomach. This fact makes a reflux even more difficult.
However, the healthy diaphragm supports this process, which is why the risk of reflux increases if a rupture occurs. The upper end of the diaphragmatic hernia may narrow, creating a so-called Schatzki ring. As a result, patients suffer from swallowing disorders or steakhouse syndrome: a piece of meat gets stuck and clogs the esophagus.
In individual cases, cramp-like pain in the upper abdomen occurs as symptoms of a diaphragmatic hernia. These arise when the hernial sac is pinched. If the opening of the diaphragm presses too hard on the worn part of the stomach, the stomach wall can be damaged. Doctors speak of Cameron's ulcer.
Paraesophageal hiatal hernia
At the beginning of a type II diaphragmatic hernia there are usually no symptoms. As the disease progresses, patients find it difficult to swallow. In some people, stomach contents flow back down the esophagus. Especially after eating, patients often feel an increased feeling of pressure in the heart area and circulatory problems. If the hernial sac twists, its blood supply is also disturbed and the sections of the stomach it contains can die. Doctors speak of an incarceration in this event, which is life-threatening.
As with the axial diaphragmatic hernia, the tissue of the stomach wall can be damaged. The defects that have arisen may bleed unnoticed. About a third of all type II hernias are therefore only discovered through chronic anemia. Doctors find the remaining two-thirds by chance or they show up as having difficulty swallowing. If a hiatal hernia causes severe symptoms, the hernial sac is usually very large. In extreme cases, the entire stomach moves into the chest cavity.
More diaphragmatic hernias
The symptoms of extraiatal diaphragmatic hernias are similar.Some patients have no symptoms whatsoever, in others these diaphragmatic hernias are more complicated. As with hiatal hernias, the contents of the hernial sac - intestinal loops or other abdominal organs - can die off and release toxins that are life-threatening for the body.
Particular care should be taken with newborns. A diaphragmatic hernia is almost always life-threatening in them. Because the trespassed parts of the abdomen displace the heart and lungs in the still small chest.
Diaphragmatic hernia: causes and risk factors
In the case of a diaphragmatic hernia, a distinction is made between the congenital and the acquired form. The latter has various causes and dimensions. Congenital diaphragmatic hernias, on the other hand, usually arise due to an incorrect development of the diaphragm.
Developmental disorders during the embryonic period
The diaphragm develops in two phases. First, a wall of simple connective tissue separates the thoracic from the abdominal cavity. Since the diaphragm is made up of two parts (septum transversum and pleuroperitoneal membrane), there is initially a gap. This closes faster on the right than on the left. In the second phase, the muscle fibers grow in. If a disorder occurs during this time (fourth to twelfth week of pregnancy), a defect occurs in the diaphragm. Through these gaps, parts of the abdomen can now shift into the chest. Since organ shells like the peritoneum are not yet formed at the beginning, the organs lie freely in the chest cavity.
Approximately seventy to eighty percent of all paraesophageal hiatal hernias are due to a congenital diaphragmatic defect. With developmental disorders of the diaphragm, there is often a large opening through which the esophagus and main artery run together (hiatus communis).
Body position as a risk factor
The axial diaphragmatic hernia is also called a sliding hernia. The contents of the abdominal cavity that have broken through can slide back and re-enter the chest cavity. So it slides back and forth between the chest and abdomen. The stomach sections shift mainly when lying down or when the upper body is lower than the lower abdomen. If those affected stand upright, the displaced parts return to the abdomen following the force of gravity.
Risk factor clenching
The likelihood of a diaphragmatic rupture increases when the abdominal muscles are tensed. This “pressing” increases the pressure in the abdomen. As a result, the stomach, which lies directly below the diaphragm, is pushed upwards through the weak or defective diaphragm. The risk increases with forced rapid exhalation, abdominal cramps and defecation.
Risk factor being very overweight and pregnancy
Similar to pressing, obesity and pregnancy also increase the risk of a diaphragmatic hernia. An excessive amount of fatty tissue in the abdomen (peritoneal fat) increases the pressure on the organs, especially when lying down. This displaces them - especially upwards. During pregnancy there is also the fact that the child growing in the uterus increasingly needs space in the abdominal cavity. The organs are pushed upwards. As a rule, such a diaphragmatic hernia regresses without any problems after the birth.
Age as a risk factor
A study from 1990 examined a connection between age and the occurrence of a diaphragmatic hernia. In people who are older than 70 years, diaphragmatic hernias can be detected on X-rays in 70 percent of cases. Experts believe that the connective tissue of the diaphragm weakens and the esophageal slit widens (blends out). In addition, the ligaments between the stomach and diaphragm loosen where the esophagus meets the stomach. As a result, the esophagus joins the stomach flatter than normal. Doctors speak of a cardiofundal misalignment or an open esophageal-stomach junction, which increases the risk of diaphragmatic hernia.
Diaphragmatic hernia: diagnosis and examination
Many hiatal hernias are discovered by chance when the doctor does an X-ray or a control gastroscopy. Usually the specialist for gastroenterology in the field of internal medicine does this, sometimes also a lung specialist (pulmonologist). Some patients suffer from heartburn with diaphragmatic hernias and should consult their family doctor with such symptoms.
Medical history (medical history) and physical examination
If a patient with diaphragmatic hernia complaints see a doctor, he asks him specifically about the symptoms that occur: how the complaints are expressed, since when and in which situations they have occurred and how they may be exacerbated. In this context, known, previous diaphragmatic hernias of the patient are particularly important.
Since traumatic events such as an operation or an accident can damage the diaphragm, such information plays a crucial role. In about 30 percent of patients, in addition to the diaphragmatic hernia, gallstone disease (cholelithiasis) and protrusions of the intestinal wall (diverticulosis) can be found. Medically, these three common diseases are called Saint-Trias. The doctor therefore also goes into the previous medical history. If loops of intestine are displaced in the diaphragmatic hernia, the doctor may be able to hear intestinal noises above the chest with the stethoscope.
Further investigations
For the exact classification and planning of a diaphragmatic hernia treatment, the doctor carries out further examinations.
|
method |
Explanation |
|
roentgen |
If you have a diaphragmatic hernia on a chest x-ray, you can often see an air bubble behind the heart and above the diaphragm. This finding points primarily to a hiatal hernia type II and III. |
|
Swallow, contrast agent |
During this examination, the patient swallows a contrast medium pulp. An X-ray is then carried out. The pulp, which is largely impermeable to X-rays, is clearly visible and shows possible constrictions which it cannot pass. Or it appears above the diaphragm in the chest area in the area of the diaphragmatic hernia. |
|
Gastroscopy (Esophagogastro-duodenoscopy, ÖGD) |
If the esophagus, stomach, and duodenum are mirrored, a diaphragmatic hernia is sometimes discovered by chance. The axial hiatal hernia then shows up as a constriction below the actual stomach entrance or the lower esophageal sphincter. This method can also be used to diagnose a significant narrowing, the Schatzki ring. A paraesophageal diaphragmatic hernia is difficult to distinguish from the mixed form. However, it is important to rule out or discover accompanying inflammation of the esophagus caused by gastric juice (reflux oesophagitis), inflammation of the stomach (gastritis) or tissue damage (ulcer). |
|
Esophageal pressure measurement |
The so-called esophageal manometry determines the pressure in the esophagus and thus provides information on possible movement disorders that can be caused by a diaphragmatic hernia. |
|
Magnetic resonance imaging (MRI) and computed tomography (CT) |
These more detailed imaging tests are particularly useful for diaphragmatic hernias that do not pass through the esophageal slit. The detailed slice representation also plays a major role in the planning of the treatment, in this case an operation. |
|
Ultrasound (of the fetus) |
In the case of a congenital diaphragmatic defect, a fine ultrasound in the unborn child shows relatively early on whether an operation is necessary. The doctor measures the relationship between the lung area and the head circumference and can thus estimate the extent of the diaphragmatic hernia. |
Diaphragmatic hernia: treatment
A diaphragmatic hernia does not always have to be treated. The axial hiatal hernia is only operated on if symptoms such as chronic reflux disease occur. The reflux of gastric juice inflames the esophagus and attacks the mucous membrane. Damage to the mucous membranes and bleeding can follow. If the reflux disease persists for a longer period of time, the risk of esophageal cancer is also significantly increased. If the mucous membrane has been damaged by a diaphragmatic hernia, surgical intervention should also be considered.
In order to avoid possible discomfort from gastric acid flowing back, appropriate medication is also prescribed. They either reduce the amount of acid (proton pump inhibitors, histamine receptor blockers) or balance the acid content (antacids).
Diaphragmatic hernia surgery
All remaining hiatal hernias are treated surgically. Because even if symptoms of a diaphragmatic hernia can appear late, the hernial sacs often enlarge more and more as the disease progresses. Doctors operate as quickly as possible in the event of complications such as disturbed food transport, a stomach twist or a trapped hernia that can quickly die as a result. In doing so, the diaphragmatic hernia that has penetrated the thoracic cavity is properly relocated back into the abdominal cavity. Then the hernia is narrowed and stabilized (hiatoplasty). In addition, the gastric fundus, i.e. the dome-shaped upper curve of the stomach, is sewn to the left underside of the diaphragm. At the end of the diaphragmatic hernia operation, the surgeons attach part of the stomach either to the anterior abdominal wall or to another part of the diaphragm (gastropexy).
If the diaphragmatic hernia surgery is only to resolve the reflux disease, the so-called fundoplication according to Nissen is carried out. The surgeon wraps the gastric fundus around the esophagus and sutures the resulting cuff. This increases the pressure on the lower esophageal sphincter at the mouth of the stomach and gastric juice can hardly flow upwards.
Plastic nets
If the diaphragmatic defect is too large, plastic nets are usually used to close the hernia gap. In particular, caution is advised in the case of congenital defects in the diaphragm. The newborns need intensive medical care, as the diaphragmatic hernia hardly allows adequate breathing. Artificial respiration is then necessary. Only when the circulation and breathing are stable can an operation be performed.
Diaphragmatic hernia: disease course and prognosis
Therapy is not necessary in approximately 80 to 90 percent of sliding hernias. And even after an operation, around 90 percent of patients with a diaphragmatic hernia are symptom-free. In newborns, the prognosis mainly depends on how limited the lung volume is. Since the diaphragmatic hernia already exists before birth, the lung on the affected side is usually underdeveloped. In severe cases, the death rate is around 40 to 50 percent.
Complications
A diaphragmatic hernia is less favorable when complications arise. If the stomach or the contents of the hernial sac twist, for example, their blood supply is cut off. As a result, the tissue becomes inflamed and dies. Toxins released as a result can spread in the body and cause severe damage (sepsis).
If large parts of the abdominal organs are displaced due to the diaphragmatic hernia, the lungs and heart are constricted in the chest. Circulatory problems and shortness of breath occur. In these cases, the operation is carried out quickly and the person concerned is cared for in an intensive care unit. In addition, bleeding from tissue damage causes chronic anemia.
change of lifestyle
Obesity and lack of exercise increase the risk of a hiatal hernia. You should therefore change your diet and lifestyle habits, i.e. you should exercise more often and eat smaller meals. It is also advisable not to eat anything right before bed. Especially with a known sliding hernia, a slightly elevated upper body at night prevents the abdominal organs from sliding up again into the chest cavity. It also reduces heartburn and reduces the risk of reflux disease and its consequences.
Because most hernias are harmless and symptom-free sliding hernias, a diaphragmatic hernia usually proceeds without complications and the prognosis is good.
Tags: news digital health anatomy











.jpg)